- Home
- About the Journal
- Peer Review
- Editorial Board
- For Authors
- Reviewer Recognition
- Archive
- Contact
- Impressum
- EWG e.V.
Cite as: Archiv EuroMedica. 2022. 12; sp: e1. DOI 10.35630/2022/12/sp.iss.1
The issue of conversion (replacement of the fixation method) is the subject of discussion, because early conversion increases the risk of infection of the surgical wound and the subsequent development of chronic gunshot osteomyelitis. However, some authors believe that the reasoned replacement of the fixation method is a key to successful rehabilitation of patients with gunshot fractures of long bones, as it creates optimal conditions for correction of bone fragments, their stable fixation and allows to begin medical rehabilitation as soon as possible. Therefore, this study is to analyze the results of treatment of gunshot fractures of long bones by using the method of conversion.
Keywords: gunshot fractures, conversion, osteosynthesis of bones, a scoring scale
Treatment of gunshot fractures of long bones is a complex and multi-stage process. The patient has to go through the path from primary fixation by extrafocal osteosynthesis to the moment of full fusion and restoration of function of the damaged limb[1]. At the same time, special importance is attached to the determination of the need to perform the conversion with the formulation of the relevant indications for the performance, as well as to its reasoned implementation [9].
Conversion is a method of treatment in the form of replacement of external fixation systems with submerged metal structures, the implementation of which depends on many factors that will be discussed in this article.
Currently, there are different concepts regarding terms and methods of conversion osteosynthesis.
Pape H, Nicholas B. and most other authors in their publications emphasize the fact that primary internal fixation is not possible in patients admitted to a medical institution with gunshot fractures of the long bones of the limbs [3].
Paderni, Pape H, Nicholas B believe that immersed osteosynthesis can be performed 1.5-2 months after the application of the external fixation device, which significantly reduces the risk of infectious complications [2].
Gianluca Testa and others point out that the definitive treatment of victims with gunshot fractures of long bones with external systems is an ideal method that gives good long-term results with a certain complication rate [4]. At the same time, in their opinion, there is no need to use open invasive surgical interventions, which can also lead to the development of infectious complications.
That is why the issue of conversion is a subject of debate, because early conversion increases the risk of infection of the surgical wound and the subsequent development of chronic gunshot osteomyelitis, and the use of external fixation devices as a method of final treatment of gunshot fractures of long bones in most cases leads to the development of contractures and functional limitations [7 ,8]. However, a justified replacement of the fixation method is a certain key to the successful restorative treatment of victims of this severe category, as it creates optimal conditions for correcting the position of bone fragments, their stable fixation, and allows the medical rehabilitation process to begin as soon as possible after receiving a combat injury, which improves the patient's quality of life [ 6].
But, unfortunately, even now, the treatment of victims with gunshot fractures of long bones is often accompanied by the development of complications: osteomyelitis (17%), persistent contractures with significant (23%) and moderate functional impairment (15%), false joints (12%), neuropathy (15%) and post-traumatic absolute shortening of limbs (10%). At the same time, the frequency of unsatisfactory functional results in this category of victims is quite significant (38%). Therefore, the issue of implementing a balanced and reasoned conversion is currently relevant and needs to be resolved [10].
Goal of the work: To analyze the results of treatment using the replacement of the fixation method during osteosynthesis in patients with combat injuries of the limbs.
Materials and methods. An analysis of the treatment of ATO/JFO for the period 2014-2021 was carried out. The number of patients with gunshot fractures of long bones was 205. The average age of the wounded was 35.3±2.32 years. Patients were divided into 2 comparison groups. The first group - 112 people, consisted of the wounded, who were converted. The second group consisted of 93 patients in whom extrafocal transosseous osteosynthesis (use of stable external rod systems and Illizarov's compression-distraction devices) was the final method of treatment.
The type of fracture according to the R.B. classification was also taken into account. Gustillo, J.T.Anderson (1984): I type was observed in 22 patients (10.7%), II – in 30 (14.6%) and III type – in 153 (74.6%): III A – 95 (62.09%), III B – 51 (33.3 %), III C – 7 (4.61 %)
The complexity of the fracture was determined using the AO classification: simple type A fractures were observed in 52 patients (18.06%), fragmentary type B fractures in 67 (32.9%), multifragmentary and segmental type C fractures in 86 (48.9% ).
Separately, it should be noted that 39.3% of upper extremity injuries were localized: gunshot fractures of the forearm were observed in 33 cases (15.9%), of the humerus in 48 (23.3%). Damage to the lower limb – 60.7%: bones of the lower leg – in 65 (32.06%), femur – in 59 (28.64%). The comparison groups did not differ (p>0.05) in terms of age, sex, clinical and nosological structure, genesis of the injury, nature and severity of gunshot wounds, and the study sample was representative.
The hospital stage of treatment of victims can be divided into 3 stages: I, IIA, II B.
During the preparation for the conversion, the first stage (stage І) is the creation of conditions for wound healing. It includes the following measures: full-fledged primary surgical treatment of wounds, adherence to the principles of second look, use of modern surgical technologies, damage control tactics, antibacterial spacers, biocomposites and reconstructive surgical interventions.
Stage II A – direct transition to replacement of the fixation method.
Hospital stage stage II B - creation of conditions for the restoration of bone tissue. The prerequisites are: stable osteosynthesis and improvement of microcirculation due to plastic surgery.
In order to evaluate the possibility of carrying out the conversion, we used the scale "Evaluation of the possibility of performing the replacement of the fixation method", which was developed by a group of authors.
This scale takes into account the specifics, nature, course of the injury, the degree of blood circulation disturbance, and the score according to their characteristics.
Attention was paid to: the size of the wound in the case of a gunshot wound, the presence of edema when planning a conversion, the duration of healing of a gunshot wound, the area of surgical intervention when planning a conversion, trophic changes in the skin of a limb, the state of the tissues of the segment in the area of the conversion, the presence of extraneous bodies.
Particular attention was paid to: accompanying pathology, structural changes in bones, the degree of inflammatory changes in the area of removed rods (spokes).
Damage to the main arteries of the segment during injury with signs of ischemia of the segment, the presence of phlebothrombosis. Important attention was paid to: the characteristics of the microflora during the initial bacteriological examination of the wound contents, the presence of positive dynamics of body temperature normalization during the treatment of the gunshot wound.
Special attention was paid to laboratory markers of inflammation when planning the conversion: the level of C-reactive protein, the absolute number of leukocytes, the ESR indicator (erythrocyte sedimentation rate). These markers of inflammation make it possible to understand the peculiarities of the pathophysiological process. The study also analyzed treatment terms, infectious complications, the nature of fracture union, the frequency of contracture development, and functional results.
Research methods: descriptive, comparative analysis, systematic approach, statistical. Statistical analysis of the information obtained during the research was carried out using the IBM SPSS Statistics Base v.22 application program package
Treatment and evacuation measures were carried out according to NATO standards. Upon admission to the medical facilities at the 2-3 level of medical care, all 205 wounded underwent primary and repeated primary surgical treatment of wounds with further stabilization of fractures by external systems.
Early stabilization of rod systems with the use of geometric triangles, rectangles and other fixing multi-plane rod modifications made it possible to use the entire necessary range of treatment measures for more reliable primary fixation, which is also an important component for the healing of gunshot wounds in average statistical terms (25-30 days) and creates conditions for further use of the conversion method.
The next step was to determine the possibility of replacing the fixation method. For this purpose, the scoring scale "Assessment of the possibility of replacing the fixation method in 2021" was developed and implemented, and the corresponding analysis was carried out (Table 1).
According to the scale: "0" - a score that characterizes confidence in performing a conversion, "1" - a score that does not significantly affect conversion planning, "2" - a score that characterizes the possible influence of this characteristic for conversion planning, "3" - a score that makes it possible to doubt the execution of the conversion, "5" - a score that indicates the impossibility of the conversion.
The final stage is summation of all obtained indicators and evaluation. Thus: an interval from 0-5 - conversion is possible, from 6-9 - questionable (summation of points does not exclude its possibility, but requires additional examination or correction of medical appointments), more than 10 - conversion is contraindicated.
| Criterion | Characteristic | Points |
| The size of the wound with a gunshot wound | Up
to 5 cm 1
stage From 5 to 10 cm 2 stage From 10 to 20 cm 3 stage More than 20 cm |
0 1 3 |
| The presence of edema when planning a conversion | Absent Minor Pastosity Moderately Pronounced Persistent Lymphostasis |
0 1 3 5 |
| Duration of healing of a gunshot wound | 20-30
days 30-40 days 40-60 days |
0 1 3 |
| Area of surgery when planning a conversion | Strong
scars Not removed sutures, openings from Extrafocal fixation Signs of inflammation of the limb segment |
0 3 5 |
| Trophic changes in the skin of the limb | Absent Mild Moderately Pronounced Trophic Ulcers |
0 1 3 5 |
| The condition of the tissues of the segment in the area of conversion | Without
features Presence of displaced flaps Scar-skin defect Muscle defect Consequences of compartment syndrome (ischemia, clinical manifestations) |
0 1 2 3 5 |
| The presence of foreign objects | Missing Small size single Small size multiple Bullet, large fragments in a section of this segment |
0 1 3 5 |
| Concomitant pathology | Varicose
veins Main blood flow disorders Diabetes mellitus: compensated form decompensated form |
1 2 3 5 |
| Structural changes in bones | Missing Signs of Local Osteoporosis Signs of Generalized Osteoporosis |
0 1 3 |
| The degree of inflammatory changes in the area of removed rods (spokes) | Missing Local Inflammatory Changes in Soft Tissues Core Osteomyelitis |
0 3 5 |
| Damage to the main arteries of the segment in case of injury with signs of segment ischemia | Missing Restoration of blood flow after damage Partial lack of blood flow (ligation of the artery) |
0 1 5 |
| Presence of phlebothrombosis | Missing PTFS Available Now |
0 3 5 |
| Characteristics of microflora during the initial bacteriological examination of wound contents | Not
detected Gram-positive microflora Gram-negative microflora MRSA |
0 2 3 5 |
| Positive dynamics of normalization of body temperature during the treatment of a gunshot wound | Available,
with a tendency to normalize Undulating Absent |
0 1 5 |
| Body temperature when planning a conversion | 36.50-36.90С 37.00-37.30С 37.40-37.70С |
0 3 5 |
| Level of total blood protein when planning conversion | 65-85
g/l 50-65 g/l for 50 g/l |
0 2 5 |
| C-reactive protein level when planning conversion | 0
– 10 mg\1 For 30 mg\1 More 30 mg\1 |
0 3 5 |
| White blood cells level when planning a conversion | Before
8 х 109 8-10 х 109 10 х109 and more |
0 3 5 |
| ESR level when planning a conversion | For
15 mm\h 15-30 mm\h More than 30 mm\h |
0 3 5 |
Table 1 Scale for assessing the possibility of replacing the fixation method
Before the conversion, the external fixation device was dismantled and a plaster cast or a skeletal extraction system was applied until the wounds healed. In addition, before planning the conversion, prevention of thromboembolic complications (elastic bandaging of the lower extremities, administration of unfractionated or low molecular weight heparins) and acute stress ulcers of the stomach and duodenum (oral or parenteral use of PPIs (proton pump inhibitors)) was carried out.
In the general distribution, patients who underwent conversion were included in group 1, which is 112, i.e. 54.6%. At the same time, the following methods of fixation were used: osseous submerged metal osteosynthesis (NMOS) in 42 (37%) cases, and blocked intramedullary osteosynthesis (BIOS) – 70 (63%).
Group 2 consisted of patients who did not undergo conversion, and the final osteosynthesis method was extrafocal osteosynthesis (use of external rod systems and Illizarov compression-distraction devices) - 93 (45.4%) (Fig. 1).
At the same time, the criteria for inclusion in the study group were patients with gunshot fractures of long bones with a bone defect of up to 6 cm. While the exclusion criteria were patients who had a bone defect of 6 cm or more and wounded with intra-articular bone defects.
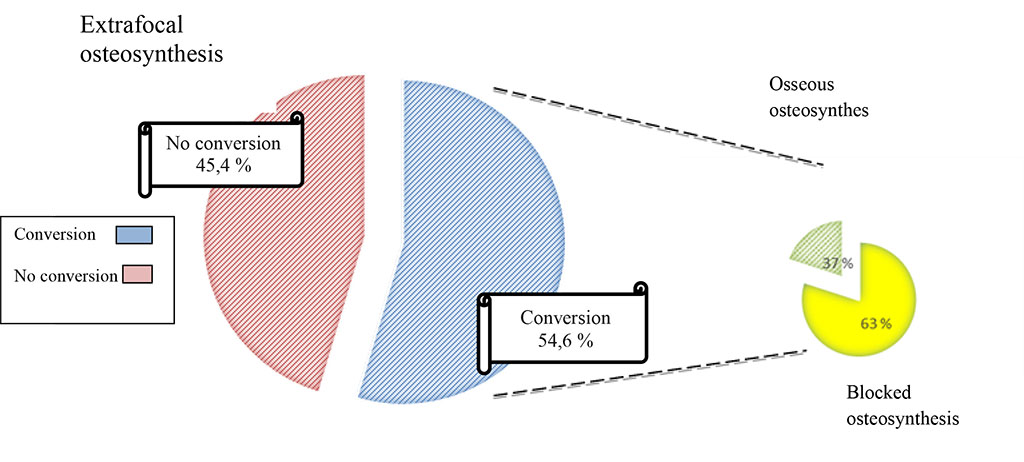
Figure 1. Distribution of conversion method in patients with gunshot fractures of long bones
In experimental group 1, for 42 patients, plates with angular stability of screws were used as fixators to replace the method. For fractures of the bones of the forearm in 11 (26.7%) cases, in 13 (31.1%) - for fractures of the humerus, in 6 (13.9%) - for fractures of the tibia and in 12 (27.9%) - for fractures of the femur. Indications for replacing the fixation method with bone osteosynthesis were unsatisfactory function of the limb, insufficient anatomical alignment of fragments and angular displacement of the main fragments, fragments behind the articular surface, in case of intra-articular fractures, the presence of a primary defect of bone tissue, delayed consolidation and formation of a false joint. It should be noted that preference was given to minimally invasive osteosynthesis from 2 small dissections without exposing the fracture zone, with preservation of blood circulation in the periosteum and more stable fixation of fragments.
In the presence of bone tissue defects, modern regenerative technologies were used: PRF and bone autospongioplasty. Based on the study and analysis of clinical materials, it was established that bone tissue defects were observed in 38 (18.2%) wounded with gunshot fractures of long bones. Free bone autospongy plastic made it possible to replace bone defects and improve the processes of osteoregeneration, reduce the likelihood of slow consolidation and the development of false joints.
In order to close soft tissue defects, myoplastic surgical interventions were used: thoraco-dorsal (38%), sural (18%), radial (15%), ulnar flap (3%), displacement of the medial or lateral head of m. gastrocnemius (23%) and m. gracilis (3%)
Blocked intramedullary osteosynthesis was performed in 70 patients. BIOS for forearm fractures was used in 11 (16.4%) cases, in 12 (17.1%) patients with humerus fractures, in 13 (17.8%) – with tibia fractures, and in 34 (48.7%) – with femur fractures. The operation was performed under the quality control of the closed repositioning of the fragments with the help of EOP (electronic optical transducer). Early final fixation of the fracture contributed to the complete restoration of the function of the limb.
Analyzing the obtained data, it is possible to see the tendency that the replacement of the fixation method was carried out mostly in patients with gunshot fractures of the hip - 46 (41.1%), and the least with gunshot injuries of the lower leg - 19 (16.9%), which is associated with the anatomical features of the muscular fascial cases of the thigh and lower leg.
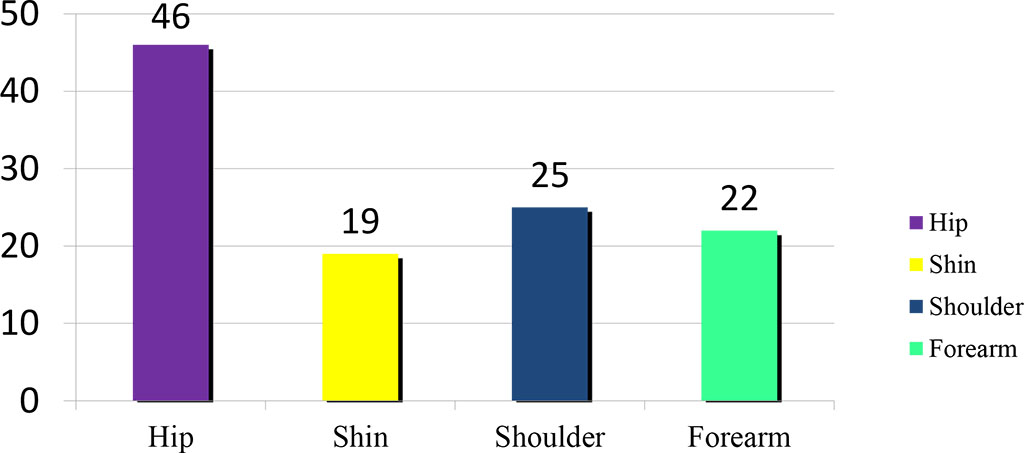
Figure 2. Structure of conversion in victims with gunshot fractures of long bones
In study group 2, stable external rod systems were used in 25 patients. For forearm fractures in 5 (20%) cases, humerus fractures in 7 (28%), tibia fractures in 4 (16%) and femur fractures in 9 (36%) cases.
The use of stable rod systems, which is achieved due to the use of fixation multi-plane rod modifications, contributes to the minimization of metal structures in tissues, the possibility of optimal repositioning in a gunshot wound and effective primary stabilization of bone fragments.
Illizarov's compression-distraction devices were used in 68 patients. For fractures of the bones of the forearm in 24 (35.2%) cases, in 4 (5%) for fractures of the humerus, in 39 (56.5%) for fractures of the tibia and in 1 (1.4%) for fractures of the femur.
Complications after the conversion of external to internal osteosynthesis were studied in 126 (61.2% of the total study sample) performed 1-3 years after the injury (Table 2).
Characteristics of complications |
Specific weight.% | Certainty. рα |
|
| Group 1 (n=72) | Group 2 (n=54) | ||
| contractures | 7.5 | 32.0 | ˂ 0.01 |
| osteomyelitis | 4.9 | 6.4 | > 0.05 |
| slow consolidation and false joint | 4.6 | 8.1 | ˂ 0.05 |
| repeated fractures | 1.9 | 2.7 | ˂ 0.05 |
Table 2. Characteristics of complications after conversion in comparison groups
The analysis of the effectiveness of the use of conversion determined a significant decrease in the terms of specialized trauma treatment by 15.3% (р<0.05), contributed to the timely union of fractures and a decrease in the development of contractures by 26.5% (р<0.01). The reason for the development of joint contractures in 4 (3.7%) of the wounded was late conversion of osteosynthesis - 1.6±0.9 months from the moment of injury.
At the same time, the functional results of the treatment of the wounded using replacement of the fixation method were studied in 126 wounded according to the complex methodology. In group 1 (72 patients), good functional results were observed in 48 (66.1%) wounded, satisfactory - in 18 (24.2%), unsatisfactory - in 6 (8.3%).
In group 2 (54 patients), good functional results were determined in 15 (27.7%) wounded, satisfactory - in 29 (54.2%), unsatisfactory - in 10 (18.1%). Thus, it was established that osteosynthesis conversion in injured with gunshot fractures of the limbs leads to an increase in good functional results from 27.7% to 66.1% and decreases the relative number of unsatisfactory cases - from 18.3% to 8.3% (р<0, 05).

|
||