- Home
- About the Journal
- Peer Review
- Editorial Board
- For Authors
- Reviewer Recognition
- Archive
- Contact
- Impressum
- EWG e.V.
Cite as: Archiv EuroMedica. 2022. 12; 6: e1. DOI 10.35630/2022/12/6.24
BACKGROUND: Dental treatment plays a big role in improving the health and quality of life of children with Down syndrome. These children need rationally organized additional dental treatment by different specialists and systematic medical observation. The high incidence and prevalence of periodontal disease in children with Down syndrome are caused by anatomical features of cranial development.
OBJECTIVE: pattern identification between anatomical characteristics and development of oral mucosal diseases in children with Down syndrome.
METHODS: The study included 24 patients with Down syndrome. They were registered at the Department of Pediatric Dentistry of the Tver Dental Polyclinic (Russia). The age of the patients was from 2 to 13 years old.
RESULTS: 59.5% of patients had a missing nasal bone. 58% of children had an arched palate. 65% of children had oral breathing type due to macroglossia and weak temporomandibular joint muscles. It can be the reason for the development of inflammatory oral mucosal diseases. The children with Down syndrome often have stomatitis and gingivitis, which develops into chronic periodontal diseases. 62% of children had the creased tongue at the age of 4 years. Down syndrome has a high prevalence of maxillofacial anomalies of up to 76%. It contributes to the formation of plaque on the teeth and caries. It often leads to damage to the rudiments of permanent teeth. The prevalence of periodontal disease in children with Down syndrome is associated with severe hypotonia of the masticatory muscles up to 87%.
CONCLUSION: Pediatric dentists focus on the features of the dental status of children with Down syndrome, taking into account the relationship of pathological processes in the maxillofacial area and somatic pathology. Specialists in pediatric dentistry must understand the importance of early prevention, which can reduce the risk of developing cavities and periodontal disease in children.
KEYWORDS: children, Down syndrome, dental treatment, periodont.
The number of disabled children in Russia increases every year according to many researchers. 728,858 disabled children were already registered in 2022. The percentage of children with disabilities in the total number of disabled people in Russia is 6.1% [1,2,5].
Down syndrome is caused by having a third copy of chromosome 21. The diagnosis is verified cytogenetically. There is currently no treatment of this chromosomal disease [1].
By the way, dental treatment plays a big role in improving the health and quality of life in children with Down syndrome. These children need rationally organized additional dental treatment by different specialists and systematic medical observation by these doctors.
The high incidence and prevalence of periodontal disease in children with Down syndrome are caused by anatomical features of cranial development (Fig. 1) and the following risk factors: local-detection of cariogenic and periodontogenic microflora; reduced hard tissue resistance; low saliva buffer capacity; poor oral hygiene and genetic, behavioral, socioeconomic factors [5]. For these reasons, the main oral disease prevention measures for children with Down syndrome should include endogenous prevention of dental diseases. The methods of exogenous prevention should be adapted to the individual psycho-emotional status of the child.
The aim is pattern identification between anatomical characteristics and development of oral mucosal diseases in children with Down syndrome.
Materials and methods. The study included 24 patients with Down's syndrome. They were registered at the Department of Paediatric Dentistry of the Dental Polyclinic of Tver. The age of the patients was from 2 to 13 years old. All documents of informed voluntary consent of research were received from all parents and legal representatives of minor children.
Results and discussions. 59.5% of patients had a missing nasal bone. A nasal cavity and an upper jaw are underdeveloped. That’s why the lower jaw protrudes forward. 58% of children had an arched palate. That’s why the mouth is usually semi-open (67%) (Fig. 2),
As a result, there are quite often vertical fissures on the lower lip, fissures in the corners of the mouth (perleche) with intense salivation, constant maceration in the corners of the mouth and a complication of streptococcal infection (Fig. 3).
The risk of oral microbiota disruption increases due to the morpho-anatomy of the oral cavity, saliva, diseases and reduced immunity. All of this can cause oral candidiasis ( Fig.4).
65% of children had oral breathing type due to macroglossia and weak temporomandibular joint muscles [4]. It can be the reason for the development of inflammatory oral mucosal diseases. The children with Down syndrome often have stomatitis and gingivitis, which develops into chronic periodontal diseases (Fig. 5).
A creased tongue is common in children with Down syndrome [1]. 62% of children had the creased tongue at the age of 4 years. There are increasing changes of the periodontal tissues in the area of the first molars and in the frontal teeth group in children with Down syndrome during their growth. It is associated with changes in the connective tissue, abnormal capillaries in the periodontium, decreased number of cell lymphocytes and abnormal activity of polymorphonuclear leukocytes [3]. Down syndrome has a high prevalence of maxillofacial anomalies of up to 76%. It is caused by dysfunction of the maxillofacial musculature. The patients usually have hypotonia of the masseter muscles, tongue and lip dysfunction and reduced oral sensitivity. This leads to incomplete chewing of food. It contributes to the formation of plaque on the teeth and caries. It often leads to damage to the rudiments of permanent teeth. The prevalence of periodontal disease in children with Down syndrome is associated with severe hypotonia of the masticatory muscles up to 87%.
Down syndrome is currently the most common disease caused by chromosomal abnormalities. Now pediatric dentists assume the features of the dental status of children with Down syndrome. They take into account the relationship of pathological processes in the maxillofacial area and somatic pathology. Specialists in pediatric dentistry must understand the importance of early prevention, which can reduce the risk of developing cavities and periodontal disease in children.
Timely treatment is essential, taking into account the dental status peculiarities unique to this category of children, which is important to consider when decontaminating the oral cavity, choosing methods and treatments. The individual program of dental disease prevention must take into account the degree of severity of somatic pathology and intellectual development of a child with Down syndrome, in order to increase the efficiency of its practical realization.
Multifaceted coverage of solutions to dental problems in children with Down syndrome is of interest to pediatric dentists, orthodontists, and surgeons.
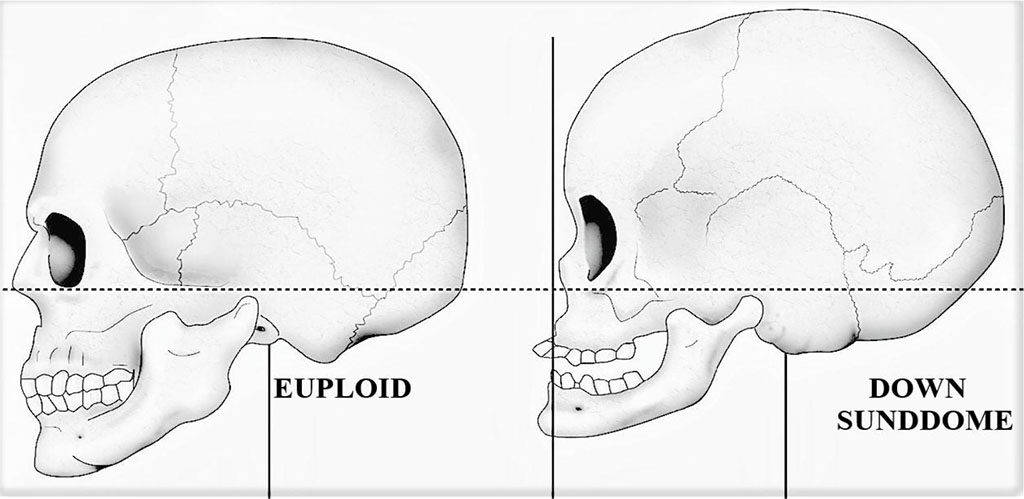
Figure 1

Figure 2
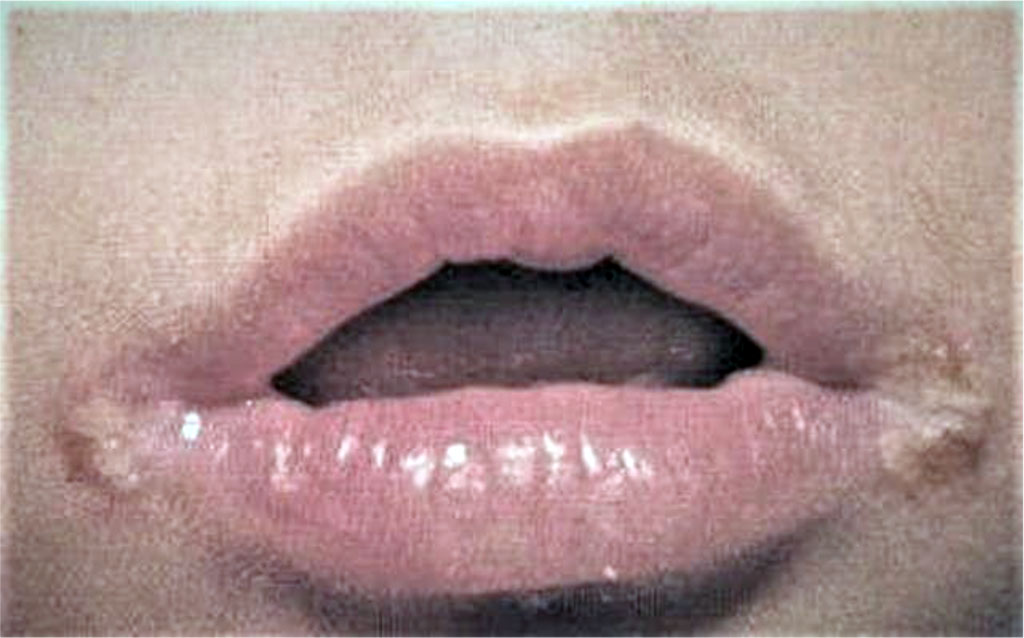
Figure 3
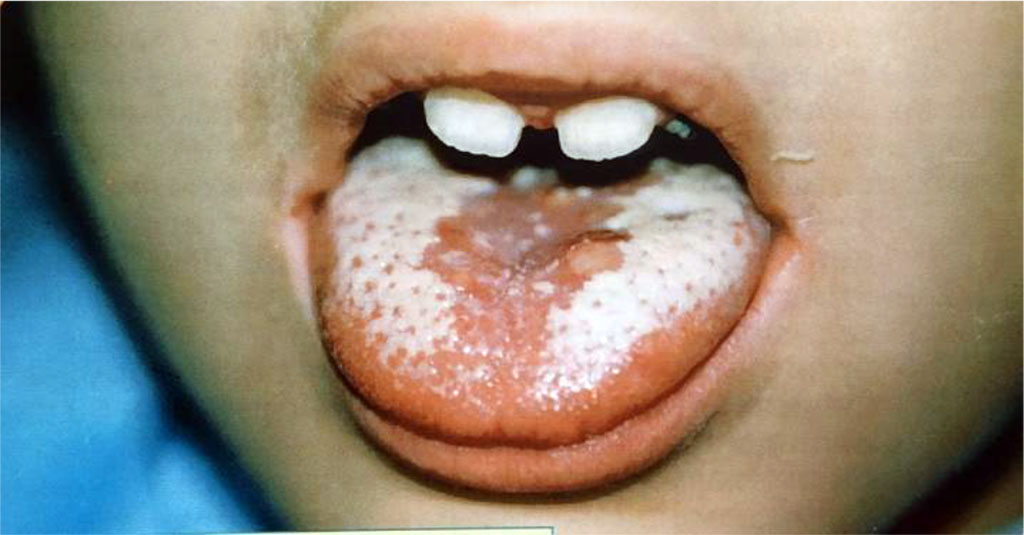
Figure 4

Figure 5

|
||