- Home
- About the Journal
- Peer Review
- Editorial Board
- For Authors
- Reviewer Recognition
- Archive
- Contact
- Impressum
- EWG e.V.
Cite as: Archiv EuroMedica. 2023. 13; 5: e1. DOI 10.35630/2023/13/5.505
In this work, the authors present a clinical case of a 65 year-old man with a history of three acute cerebrovascular accidents similar to a transient ischemic attack and/or ischemic stroke with a minor neurological deficit with short-term weakness in the left or right limbs and loss of coordination. Carotid angiography showed that the blood supply to the brain was provided by a single internal carotid artery on the left and a potent collateral network on the same side. The patient underwent stenting of the internal carotid artery on the left. As a result, blood supply was restored through the stented artery and pronounced collateralization on the right. This clinical case demonstrated that even in complex clinical situations associated with multifocal lesions of the carotid arteries, the use of x-ray endovascular technologies can achieve good clinical results, and x-ray-guided endovascular treatment of critical stenosis of the solitary internal carotid artery will allow achieving significant regression of neurological deficit and designating prognosis optima.
Keywords: carotid artery stenosis, carotid artery stenting, cerebrovascular disease, x-ray angiography, multifocal stenosis, collateral cerebral circulation
Atherosclerosis ranks first globally in terms of arterial damage and is a leading cause of death among cardiovascular pathologies. In recent decades, cerebral stroke has consistently held second place among other causes of death, second only to coronary heart disease. Damage to the internal carotid arteries by the atherosclerotic process causes a high risk of developing ischemic stroke, and there is a direct connection between the degree of stenosis and the risk of acute cerebrovascular accident. A clinically significant manifestation of arterial atherosclerosis is the damage to cerebrovascular or brachiocephalic vessels, which leads to transient ischemic attack or cerebral infarction. The incidence of cerebral infarction in the European Union is 0.2% of the total population and amounts to about 1.4 million cases per year [1, 2].
However, there is significant variability in the causes, as well as the clinical manifestations of systemic damage to the cerebral arteries – from asymptomatic disease course to sudden fatal outcome. In individual patients, cerebral perfusion depends not only on the degree of stenosis, but also on the patency of collateral pathways. Collateral circulation is an important aspect of cerebral circulation, which affects the risk of ischemic stroke, as well as the characteristics of its manifestation, the nature of neurological symptoms, and the severity of cognitive impairment. Several collateral pathways may contribute to cerebral perfusion in patients with severe carotid artery disease. Collateral flow through the circle of Willis is considered the primary collateral pathway. These collaterals consist of cross-flow through the anterior communicating artery towards the hemisphere, ipsilateral to the most severely affected internal carotid artery: blood flow from the posterior to the anterior segment through the ipsilateral posterior communicating artery, or of both of these systems [4].
X-ray-guided endovascular carotid stenting in patients with atherosclerotic lesions of the internal carotid artery, presenting a high surgical risk group, has confirmed its high efficiency and safety [5-8]. Stenting in patients with repeated stenosis of the internal carotid artery after previous carotid endarterectomy or multifocal critical lesion of the internal carotid artery is the method of choice [9-12].
Patient K., a 65 years old man was admitted to the department of x-ray endovascular surgery with complaints of headache, dizziness, and tinnitus. Syncope occurs occasionally. Anamnesis revealed that the patient had suffered 3 acute cerebrovascular accidents of the type of transient ischemic attack and/or ischemic stroke with a minor neurological deficit with short-term weakness in the left or right limbs and loss of coordination 2, 4 and 5 years ago. Physical neurological status. Consciousness is clear. No meningeal signs. Cognitive functions are slightly reduced. D, S symptoms of oral automatism. Right-handed. Emotionally labile. Pupils D = S. The reaction of the pupils to light is lively. Movement of the eyeballs is limited outward. Convergence is weakened. Nystagmus and diplopia are not defined. Mild paresis of the facial muscles on the left. Pharyngeal reflexes are alive D = S. Slight deviation of the tongue to the right. 4 points right-sided hemiparesis. Right-sided mild hemihypesthesia. Tendon reflexes D > S. Babinski and Rossolimo signs are positive on the right. Romberg's test shows staggering. Coordinating tests revealed slight past-pointing and intention on the right. Pelvic functions under control.
Carotid angiography shows that the blood supply to the brain is provided by a single internal carotid artery on the left and a potent collateral network on the same side. Intracranially, both hemispheres are supplied with blood from one side. Fig. 1.

Fig. 1. Carotid angiography. Stenosis of the internal carotid artery on the left (91%), visible collaterals
Diagnosis: Atherosclerosis of the brachiocephalic arteries. Occlusion of the internal carotid artery on the right. Subocclusion of the internal carotid artery on the left (91%). Chronic cerebrovascular insufficiency of the 4th degree (according to A.V. Pokrovsky) [13]. Condition after three ischemic strokes.
The purpose of the upcoming operation is to correct neurological deficits and prevent further development of strokes. Name of the operation: transluminal balloon angioplasty of the left internal carotid artery with stenting. Surgery protocol: under local anesthesia with Sol. Lidocani 2%-2 ml., the common femoral artery on the left was punctured and catheterized. A 6F introducer was installed and subsequently replaced with an 8F one. A guiding catheter was installed at the mouth of the common carotid artery on the left; a conductor with an Embosheld NAV6 filter was inserted beyond the stenosis site into the intracranial section of the internal carotid artery and opened. A 40 mm Protégé RX Tapered 10-7 self-expanding peripheral stent was implanted in the stenosis site. Next, postdilatation of the stenosis site was performed using a 20 mm RX Viatrac 14 Plus 6.0X balloon catheter with a pressure up to 10 atm. A control cerebral angiogram had no signs of malposition, proximal or distal dissection, and no distal embolism was detected. The tools were removed. A pressure bandage was applied. As a result of the operation, blood supply through the stented artery and pronounced collateralization on the right was restored. Fig. 2. Neurological status after surgical treatment showed significant positive dynamics. Consciousness is clear. No meningeal signs. Cognitive functions are preserved. D, S symptoms of oral automatism. Emotional lability is not detected. Pupils D = S. The reaction of the pupils to light is lively. The movements of the eyeballs are slightly limited outward. Convergence is weakened. Nystagmus and diplopia are not detected. Mild paresis and facial asymmetry. Pharyngeal reflexes are alive D = S. The tongue is in the midline. Paresis and sensory disorders are not detected. Tendon reflexes D>S. Babinski and Rossolimo signs are positive on the right side. Stable in the Romberg test. Coordination tests are successful. Pelvic functions under control.
The patient was discharged from the department in satisfactory condition and had no complaints.
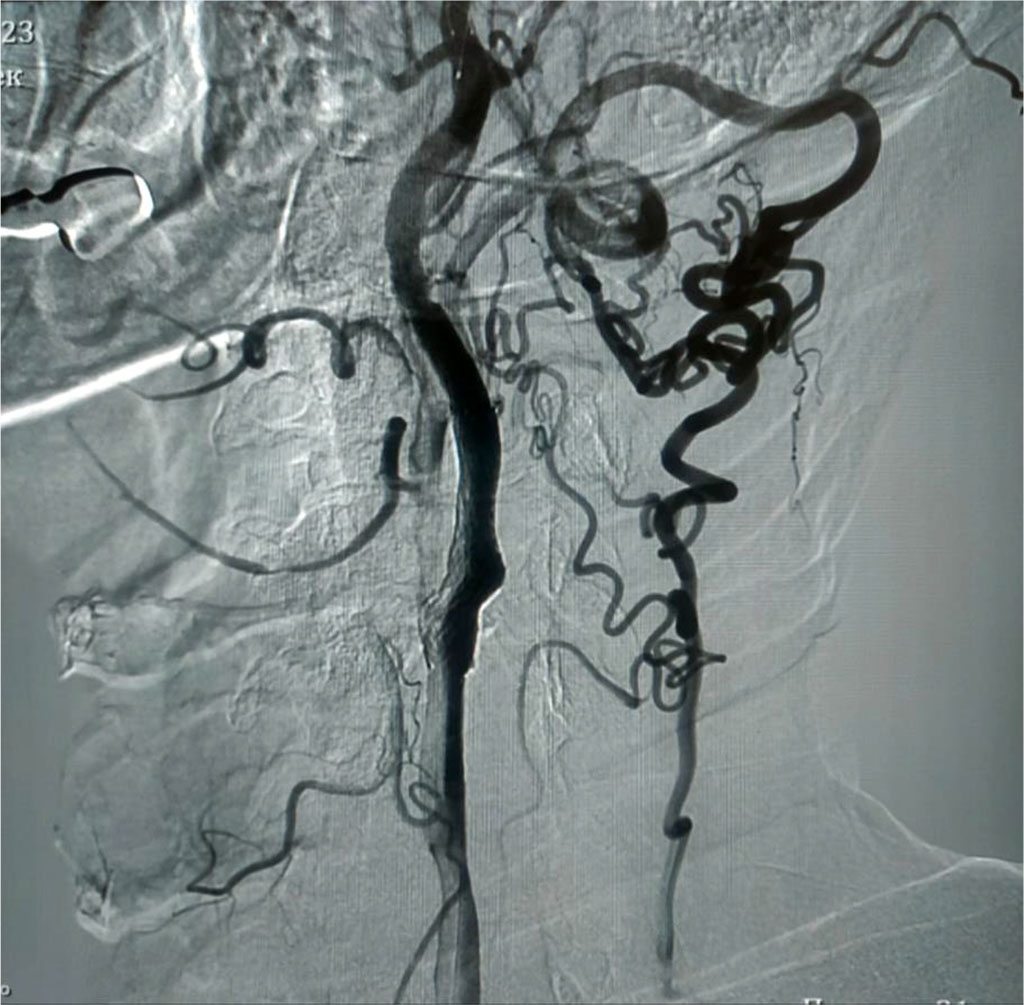
Fig. 2. Carotid angiography. Condition after x-ray-guided endovascular stenting of the internal carotid artery on the left.
Thus, this clinical case demonstrated that even in complex clinical situations associated with multifocal lesions of the carotid arteries, the use of x-ray endovascular technologies can achieve good clinical results. Specifically, X-ray-guided endovascular treatment of critical stenosis of the solitary internal carotid artery has resulted in significant regression of neurological deficit and designating prognosis optima.

|
||