Erfolgreich durch internationale Zusammenarbeit
dentistry
Cite as: Archiv EuroMedica. 2022. 12; 4: e1. DOI 10.35630/2199-885X/2022/12/4.14
Received
28 May 2022;
Received in revised form 20 June 2022;
Published 4 July
2022
X-RAY
CEPHALOMETRIC FEATURES OF NASAL AND GNATHIC SECTIONS IN DIFFERENT
FACIAL SKELETON GROWTH TYPES
Dmitry
Domenyuk1,5 
 ,
Taisiya Kochkonyan2 ,
,
Taisiya Kochkonyan2 ,
Vladimir Shkarin3 ,
Sergey Dmitrienko3 ,
Stanislav Domenyuk4
1 Stavropol
State Medical University, Stavropol;
2 Kuban
State Medical University, Krasnodar;
3 Volgograd
State
Medical University, Volgograd;
4 North
Caucasus Federal University, Stavropol;
5Pyatigorsk
Medical and Pharmaceutical Institute − Branch of the Volgograd
State Medical University, Pyatigorsk, Russia
 download article (pdf)
download article (pdf)
domenyukda@mail.ru
Abstract
Based
on the results obtained through studying head lateral
teleroentgenograms of 68 patients (aged 18−25)
with a full set of permanent teeth and physiological occlusion, a
method was developed, which allows exploring the angular parameters
of the nasal (n-cond-sn) and gnathic (sn-cond-gn) face sections. In
view of the type of the face gnathic part growth, the patients were
divided into three groups: Group 1 (n=27) included patients with a
neutral type of face growth and a mandibular angle of 119°−123°.
Group
2 (n=22) were patients featuring a vertical type of the face gnathic
part growth with a mandibular angle exceeding 123°. In patients of
Group 3 (n=19), the mandibular angle was below 119° along with the
horizontal type of the face gnathic part growth. Patients with
physiological occlusion were found to have the nasal part angular
parameters (n-cond-sn) relatively stable at different types of jaw
growth: neutral type, 29.85±0.22°; vertical type, 30.01±0.22°;
horizontal type, 29.96±0.29°, respectively. The angular parameters
of the face gnathic part (sn-cond-gn) are variable and were
identified based on the type of face growth, whereas the dimensional
parameters in case of the vertical growth type (33.02±0.26°) exceed
similar indices in people who featured the neutral (30.04±0.28°)
and horizontal (26.92±0.29°) growth types. The
angular parameters obtained for the nasal (n-cond-sn) and gnathic
(sn-cond-gn) parts of the face can be employed as stable reference
points when assessing the jaw growth types in patients with
physiological occlusion, detecting facial features with maxillofacial
anomalies and deformities (both congenital and acquired), and serve
as a criterion pointing at the effectiveness of prosthetic and
orthodontic treatment.
Keywords:
X-ray cephalometry, face nasal part, gnathic part of face, facial
part of skull, head lateral teleroentgenography, facial skeleton
growth types.
INTRODUCTION
The
normal variability of morphological features of the human
craniofacial region, as well as the structure and the patterns of
their development are of reasonable research and applied interest for
experts in the area of clinical dentistry, orthodontics,
maxillofacial surgery, neurosurgery, and ophthalmology [21,49,54].
The
constitutionally meaningful features of the facial section taken as
objects for in-depth study within aesthetic dentistry include: the
gnathic type of the face (meso-, dolicho-, brachygnathic); the type
of the facial skeleton growth (neutral, horizontal, vertical); the
masticatory muscles thickness and spatial orientation; the
morphological (angle) and morphometric features of the mandible
(condylar width, angular width) [4,15,22,28,33,37,39]. Analysis of
orthodontic treatment outcomes in patients with maxillary system
issues, which is aimed at ensuring proper morphometric, functional
and aesthetic balance, is performed in various aspects: the
evaluation of the anatomical and functional status of the
maxillofacial area, of the occlusion, and of aesthetic effect
achieved [5,9,14,16,24,31,41,52,58].
The
diagnostic value of identifying the facial skeleton growth type roots
in the fact that patients have high demands concerning orthodontic
treatment, while paying special attention to aesthetics. High-quality
planning and treatment take an orthodontist knowing not only the
normal indicators, yet also respective deviations from such values,
including variations in view of the facial skeleton growth type
[3,6,29,40,59].
The
authors prove that the facial skeleton growth type developed in
childhood determines the further direction for the growth of the face
gnathic part, while horizontal and vertical growth types point at
predisposition to developing dental issues [1,18,35,51,53,61].
Subject
to research outcomes, clinicians have developed the parameters of the
norm, identified the distinctive features of the facial skeleton
structure for the orthognathic bite depending on the gender and the
age, the morphology of the temporomandibular joint, the dental
arches, the occlusal plane, and the teeth position [8,12,38,43,62].
There has been an interconnection detected between the lateral teeth
group mesiodistal tilt of the upper and lower jaws in people
featuring different types of facial skeleton growth, and for various
physiological occlusions [25,27,42,34,50,60].
The
orthognathic bite, recognized as a standard norm when investigating
the etiopathogenesis of dental issues, is described as dominated by
the neutral type of face growth. The orthognathic bite reveals quite
wide variability range, where the height and the depth may vary
significantly, the general structure of the facial skeleton, though,
remaining within the neutral type of growth. In case of the neutral
growth type, the height and the depth of the facial skeleton feature
approximately similar development [7,11,20,48].
The
depth predominance over the height is typical of the horizontal
growth type, whereas the height prevailing means that the growth type
is vertical. In these cases, we are talking about disturbed
proportions in the facial skeleton development in the
transverse-longitudinal directions, which affects the majority of the
craniofacial structures. In case of the horizontal growth type, for
instance, there is anterior rotation of the upper jaw, as well as an
increase in the incisors protrusion, and a decrease in the alveolar
process height in the posterior part to be observed. The vertical
type of growth features a posterior rotation of the upper jaw, an
increase in the face total height as well as in the height of the
face middle zone, and the lower jaw micrognathia [44,46,55].
Literature
contains some data on face nasal parameters deviations from the age
norm in people with congenital pathology and in case of
genetics-related health issues diseases [2,23,45].
Cephalometric
studies that are part of the mandatory diagnostic measures employed
to examine patients with dental issues are of specific interest in
applied dentistry, since they allow shaping an objective view of the
skull parameters and their relationships [10,17,57].
Craniometric
and cephalometric studies allow not only identifying the
face-soft-tissue-to-bone-structure ratio, but monitoring the
effectiveness of orthodontic and surgical treatment, too
[19,32,36,56]. Experts have found the facial skull bone structures to
have craniological polymorphism, as well as to determine its relief
and symmetry in relation to the median sagittal plane, thus working a
significant effect on both the facial aesthetics and the face profile
harmony [13,26,30,47]. An analysis of respective literature shows
that angular measurements characterizing the X-ray cephalometric
features of the facial skeleton nasal and gnathic sections in
patients with physiological bites are lacking, which explains the
reason behind this present study.
Aim
of study: to
carry out a comparative analysis of the angular parameters of the
face nasal and gnathic sections on a lateral teleroentgenograms
obtained from young people with physiological occlusions.
MATERIALS
AND METHODS
X-ray
studies involved 68 young people aged 18−25, with a full set of
permanent teeth and physiological types of occlusal relationships.
Prior to the research, voluntary informed consents were obtained
subject to the Ethical
Principles for Medical Research Involving Human Subjects
(Nuremberg Code, 1947; World Medical Association Declaration of
Helsinki, 1964). The patients were divided into three groups based on
the type of face gnathic part growth. Group 1 were 27 persons with a
neutral type of facial growth, where the mandibular angle was
119°−123°. The patients belonging to Group 2 (n=22) featured the
vertical type of the face gnathic growth and an increase in the
mandibular angle (above 123°). In Group 3 (n=19), a horizontal type
of growth of the face gnathic part was to be observed along with a
decrease in the mandibular angle (under 119°) (Fig.1).
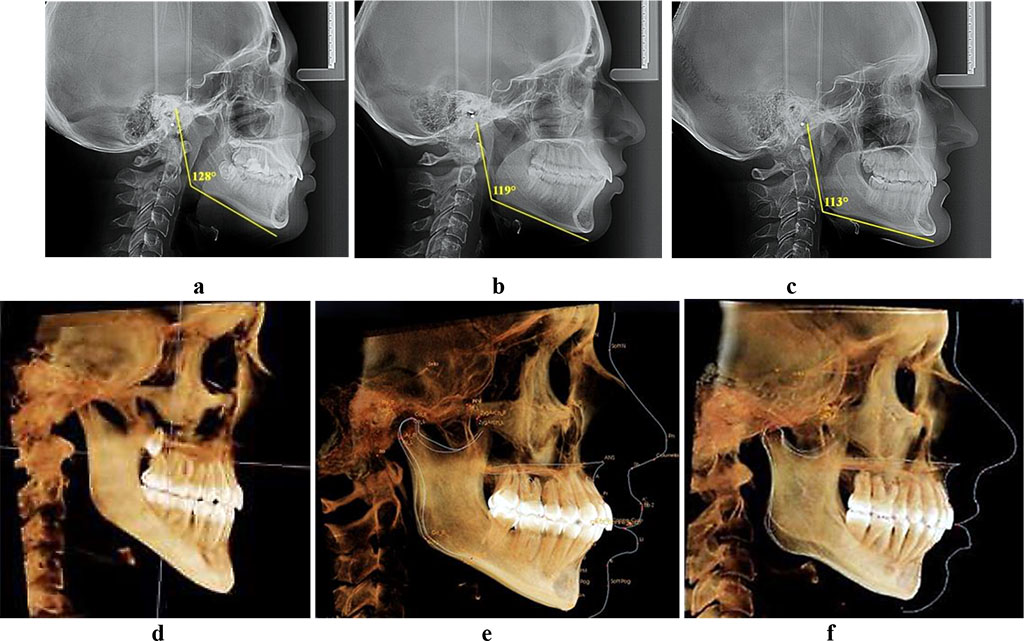
Fig.
1. Teleroentgenograms and computed tomograms, patients with vertical
(a, d), neutral (b, е)
and horizontal (c, f) type of jaw growth.
On
the lateral teleroentgenogram, the main reference point was the top
point of the lower jaw articular head, which was marked as the cond point (condylion).
The cutaneous point of n (nasion) was placed in the deepest spot between the forehead and the
nose. The sn (subnasale)
point was located at the junction spot of the nasal septum and the
upper lip. The cutaneous gn (gnation)
point was recognized to be the most prominent point of the chin soft
tissues protruding forward and downwards. These points were connected
by horizontal lines drawn from the articular point while shaping
nasal (n-cond-sn)
and gnathic (sn-cond-gn)
angles (Fig. 2).
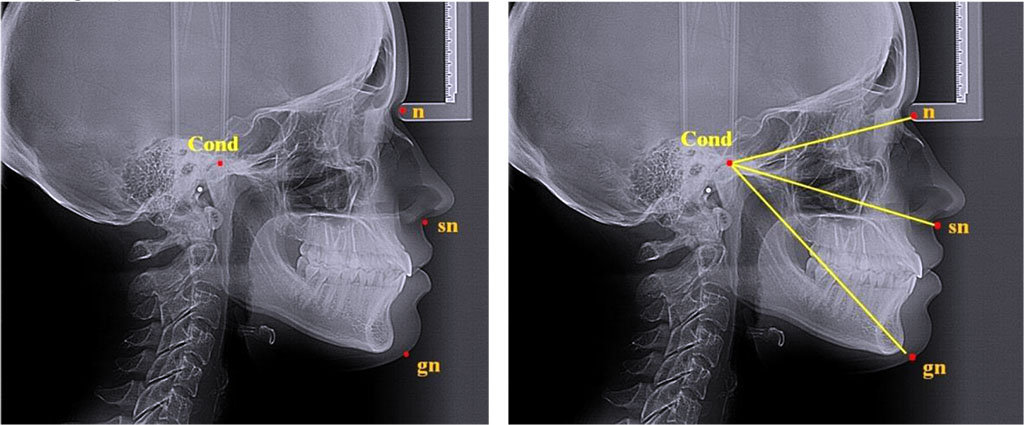
Fig.
2. Major reference points for analyzing nasal and gnathic face parts
on teleroentgenograms, lateral projection
The
teleroentgenograms were used to match the resulting angles shaped by
the said lines.
The
statistical data processing was performed using the Microsoft Excel
2013 software and the SPSS Statistics 22.0 software package. The
calculated values included the median value (M), the non-sampling
error (± m) while taking into account the mean square deviation (δ).
The minimal statistically significant difference was set at p<0.05.
RESULTS
AND DISCUSSION
In
people featuring physiological occlusions, in case of the neutral jaw
growth type (Group 1), the mandibular angle was 120.97±0.38 degrees
(δ=1.96).
The
face nasal angle (n-cond-sn) within the group was an average of
29.85±0.22 degrees (δ=1.15),
the gnathic angle (sn-cond-gn) being 30.04±0.28 degrees (δ=1.44).
Given
the above, as could be seen from the teleroentgenograms, young people
with physiologically occlusive relationships and the neutral type of
gnathic growth, the angular parameters of the face gnathic part
matched similar parameters of the nasal part, while no statistically
significant differences (p<0.05) between the parameters in focus
were detected (Fig. 3).
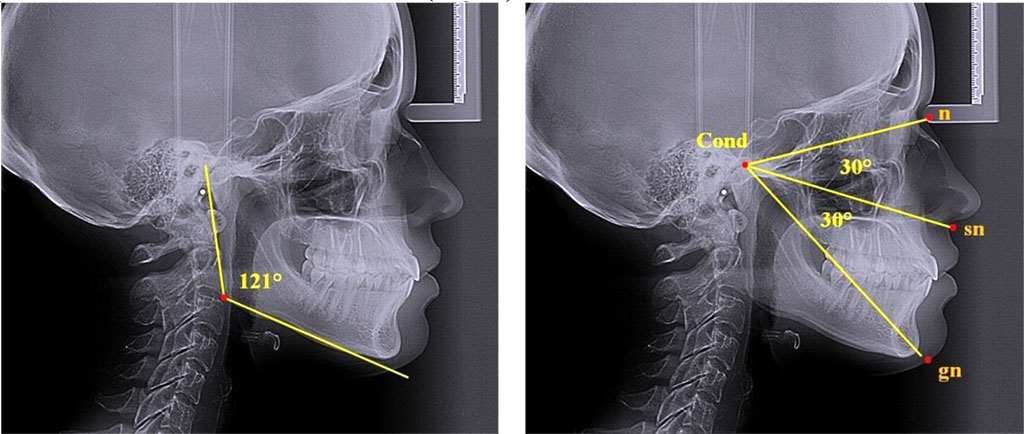
Fig.
3. Angular parameters, nasal and gnathic part of face;
teleroentgenograms, lateral projection; neutral type of growth
In
patients with physiological occlusions and the vertical jaw growth
(Group 2), the mandibular angle was 128.36±0.51 degrees (δ=2.39),
which exceeded reliably (p<0.05) the similar parameter in those
who featured the neutral type of the gnathic growth of face. An
increase in the non-sampling error and in the mean square deviation
were indicative of a greater variability in the mandibular angle if
compared to the neutral type of growth.
The
nasal facial angle (n-cond-sn) in patients with the vertical jaw
growth was 30.01±0.22 degrees (δ=1.05).
There were no significant differences observed pertaining to this
parameter, if compared with the results obtained in Group 1 (p>0.05),
which means that the type of the face gnathic part does not have any
effect on the indicators related to the nasal part of the face. The
gnathic angle value (sn-cond-gn) in patients of Group 2 was
significantly above that in patients of Group 1 (p<0.05), making
up 33.02±0.26 degrees (δ=1.23).
Besides, the angle of the gnathic part exceeded the nasal angle by 3
degrees (Fig. 4).
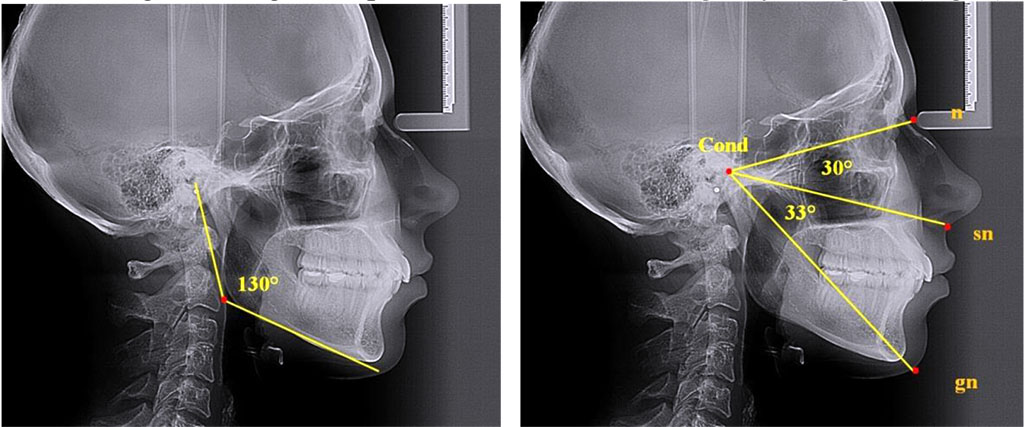
Fig.
4. Angular parameters, nasal and gnathic parts of face;
teleroentgenograms in lateral projection, vertical growth type
This
means that in case of the vertical growth type of the face gnathic
part observed in young people with physiological occlusal
relationships, the angular parameters of the gnathic part were
significantly above similar parameters of the nasal part (р˃0.05).
In
patients with the physiological types of occlusion and the horizontal
jaw growth (Group 3), the mandibular angle was 111.89±0.59 degrees
(δ=2.52),
which is significantly below (p<0.05) that in people with the
neutral type of gnathic face growth. An increase in the non-sampling
error and in the mean square deviation, just like in Group 2, pointed
at a greater variability of the mandibular angle than in case of the
neutral type of growth of the face gnathic part. The nasal facial
angle (n-cond-sn) in patients with the horizontal jaw growth was
29.96±0.29 degrees (δ=1.23).
There were no significant differences detected in this parameter
compared with the data obtained from studying Groups 1 and 2
(p>0.05), which confirms the idea that the type of the gnathic
part has no effect on the face nasal part parameters. The gnathic
angle (sn-cond-gn) in patients with the horizontal jaw growth and
significantly smaller than in people with the neutral type of the
face gnathic growth (p<0.05), and was 26.92±0.29 degrees
(δ=1.24).
Besides, the face gnathic part angle was smaller than the nasal angle
by 3 degrees (Fig. 5).
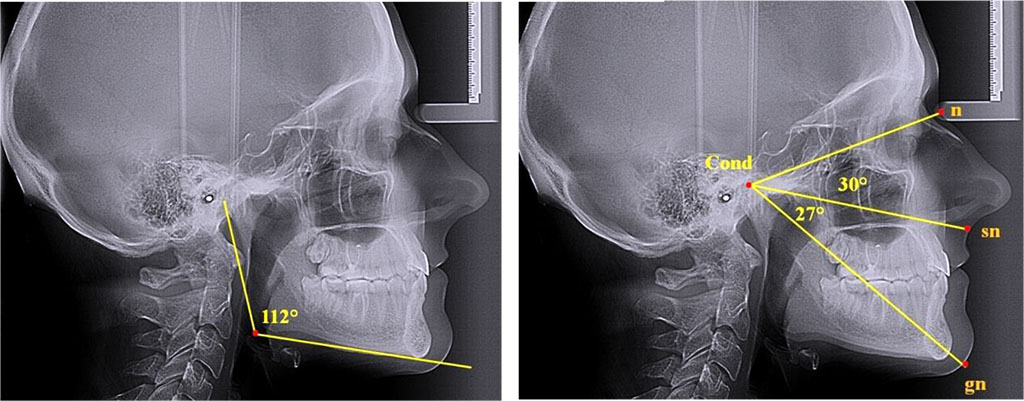
Fig.
5. Angular parameters of nasal and gnathic part of face;
teleroentgenograms, lateral projection; horizontal growth type
The
obtained angles of the face nasal and gnathic sections can serve as
reference points when assessing the jaw growth type in case of
physiological occlusion, detecting the facial features bearing
maxillofacial anomalies and deformities (either congenital or
acquired genesis), as well as be employed as a criterion to evaluate
the effectiveness of prosthetic and orthodontic treatment.
CONCLUSIONS
- The
X-ray morphometric measurements of head teleroentgenograms in the
lateral projection are reliable and informative when it comes to
studying the size and location of the skull facial bones, the main
directions of head facial growth, as well as when analyzing the
angular parameters of the nasal and gnathic parts of the face.
- The
head facial part types of growth are determined by the basic linear
and angular parameters of teleroentgenograms, as well as by the main
jaw growth types.
- Given
the regularities pertaining to the skull facial structure,
dependencies observed between the morphometric parameters of the
dental arches, jaws, facial skeleton bones, as well as the
relationship of stable anatomical references of the craniofacial
complex with certain planes, there was a method proposed for studying
the angular parameters of the face nasal and gnathic parts on head
lateral-projection teleroentgenograms.
- Measuring the angular parameters of the nasal (n-cond-sn) and the
gnathic (sn-cond-gn) sectors of the skull facial part on
teleroentgenograms (lateral projection of the head), the condylion bone point and the soft-tissue (skin) points of n (nasion), sn (subnasale),
and gn (gnation)
were used as anthropometric references.
- The proposed method employed to study the facial skeleton using
stable anthropometric references shows that patients with
physiological occlusion have angular parameters of the face nasal
part (n-cond-sn)
that are relatively stable at various types of jaw growth, making up:
the neutral type, 29.85±0.22°; for the vertical type, 30.01±0.22°;
for the horizontal type, 29.96±0.29°.
- The
angular parameters of the facial skull gnathic part ( sn-cond-gn)
are variable and are determined by head facial growth, while the
dimensional parameters in case of the vertical growth type
(33.02±0.26°) go beyond similar values in people with the neutral
(30.04±0.28°) and the horizontal (26.92±0.29°) growth types.
- The
angular value of the face nasal part ( n-cond-sn)
can be well used in clinical dentistry for identifying occlusion
issues in the vertical plane, both in the nasal and in the gnathic
parts of the face.
REFERENCES
- Ash
M.M. Wheeler’s dental anatomy, physiology and occlusion. Philadelphia:
WB Saunders; 2003.
- Avanisyan
V., Al-Harazi G. Morphology
of facial skeleton in children with undifferentiated connective
tissue dysplasia.
Archiv EuroMedica. 2020. Vol. 10; 3: 130-141. https://dx.doi.org/10.35630/2199-885X/2020/10/3.32
- Becker
I. M. Comprehensive Occlusal Concepts in Clinical Practice / I. M. Becker.
– John Wiley & Sons, 2010. – 316 p.
- Bennett
J. C., McLaughlin R. P. Orthodontic management of the dentition with the preadjusted
appliance / J. C. Bennett, R. P. McLaughlin. – Isis Medical Media,
1997. – 380 р.
- Bisharа,
S.E. Textbook of Orthodontics. Mosby. – 2001. − 592 р.
- Burstone,
C.J. Physics and clinical orthodontics: 100 years ago and today [Text] /
C.J. Burstone // Am J Orthod Dentofacial Orthop. – 2015. Mar. –
147(3). – Р.
293-4.
DOI: 10.1016/j.ajodo.2014.12.011.
- Carlson,
James E. Physiologic occlusion [Text] / James E. Carlson. – UK: – St
Louis: Mosby, 2009. –218 р.
- Clark
J.R. Functional occlusion: I. A review / J.R. Clark, R.D. Evans // J.
Orthod. - 2001. - Vol.28, No 1. - P.76-81.
DOI: 10.1093/ortho/28.1.76
- Davydov
B.N., Budaychiev G.M-A. Changes of the morphological state of tissue of the paradontal
complex in the dynamics of orthodontic transfer of teeth
(experimental study). Periodontology,
2018; Vol. 23; 1-23(86): 69-78. DOI:10.25636/PMP.1.2018.1.15
- Davydov
B.N. Improving diagnostics of periodontal diseases in children with
connective tissue dysplasia based on X-ray morphometric and
densitometric data. Periodontology.2020;25(4):266-275.
(in Russ.) https://doi.org/10.33925/1683-3759-2020-25-4-266-275.
- Dawson
P.E. Functional
Occlusion: From TMJ to Smile Design / P. E. Dawson. – Elsevier
Health Sciences, 2006. – 647 p.
- Dmitrienko
S.V. Enhancement of research method for spatial location of
temporomandibular elements and maxillary and mandibular medial
incisors. Archiv
EuroMedica.
2019. Vol. 9; 3. P. 38-44. https://doi.org/10.35630/2199-885X/2019/9/1/38
- Dmitrienko
T.D. Connection between clinical and radiological torque of medial
incisor at physiological occlusion. Archiv
EuroMedica.
2019. Vol. 9. № 1. P. 29-37. https://doi.org/10.35630/2199-885X/2019/9/1/29
- Domenyuk
D.A., Kochkonyan T.S., Shkarin V.V.
Conceptual
approach to diagnosing and treating dentoalveolar transversal
divergent occlusion. Archiv
EuroMedica.
2022. 12; 3: e1. DOI 10.35630/2022/12/3.25
- Domenyuk
D.A., Kochkonyan T.S. Implementation of neuromuscular dentistry principles in
rehabilitation of patients with complete adentia. Archiv
EuroMedica. 2022.
Vol. 12; 2: 108-117. https://doi.org/10.35630/2199-885X/2022/12/2.29
- Domenyuk
D.A., Lepilin А.V., Fomin I.V. Improving
odontometric diagnostics at jaw stone model examination. Archiv EuroMedica.
2018. Vol. 8; 1: 34-35. https://doi.org/10.35630/2199-885X/2018/8/1/34
- Domenyuk
D.A. Major
telerenthengogram indicators in people with various growth types of
facial area. Archiv EuroMedica.
2018. Vol.
8; 1: 19-24. https://doi.org/10.35630/2199-885X/2018/8/1/19
- Domenyuk D.A., Vedeshina E G., Dmitrienko S.V. Mistakes
in
Pont
(Linder-Hart)
method
used
for
diagnosing
abnormal
dental
arches
in
transversal
plane. Archiv
EuroMedica.
2016. Vol. 6; 2: 23-26.
- Domenyuk
D. Structural
arrangement of the temporomandibular joint in view of the
constitutional anatomy. Archiv
EuroMedica.
2020. Vol.
10. № 1. Р.
126-136. https://doi.org/10.35630/2199-885X/2020/10/37
- End
E. Physiological Occlusion of Human Dentism: Diagnosis & Treatment
/ E. End. – Verlag Neuer Merkur GmbH, 2006. – 192 p.
- Epker
B. N., Fish L. C., Stella J. P. Dentofacial deformities: integrated orthodontic and surgical
correction / B. N. Epker, L. C. Fish, J. P. Stella. – Mosby St.
Louis, 1995. – 656 р.
- Fomin
I.V. Effect of jaw growth type on dentofacial angle in analyzing lateral
teleradiographic images. Archiv
EuroMedica.
2019. Vol. 9; 1: 136-137. https://doi.org/10.35630/2199-885X/2019/9/2/136
- Fischev
S.B., Puzdyryova M.N. Morphological
features of dentofacial area in peoples with dental arch issues
combined with occlusion anomalies. Archiv EuroMedica. 2019. Vol. 9;
1: 162-163. https://doi.org/10.35630/2199-885X/2019/9/1/162
- Ghamdan
Al.H. A
method for modeling artificial dentures in patients with adentia
based on individual sizes of alveolar arches and constitution type. Archiv
EuroMedica.
2021. Vol. 11; 1: 109–115. https://doi.org/10.35630/2199-885X/2021/11/1.25
- Ghamdan
Al.H. Occlusal
plane orientation in patients with dentofacial anomalies based on
morphometric cranio-facial measurements. Archiv
EuroMedica.
2021. Vol. 11; 1: 116–121. https://doi.org/10.35630/2199-885X/2021/11/1.26
- Graber
L. W., Vanarsdall R. L., Vig K. W. L., Huang G. J. Orthodontics:
Current Principles and Techniques. – Elsevier, 2016. – 928 p.
- Grinin
V.M., Khalfin R.A. Specific features of grinder teeth rotation at physiological
occlusion of various gnathic dental arches. Archiv
EuroMedica.
2019. Vol. 9; 2: 168-173. https://doi.org/10.35630/2199-885X/2019/9/2/168
- Grinin
V.M., Khalfin R.A. Specific features of transversal and vertical parameters in lower
molars crowns at various dental types of arches. Archiv
EuroMedica.
2019. Vol. 9; 2: 174-181. https://doi.org/10.35630/2199-885X/2019/9/2/174
- Harutyunyan
Yu. Undifferentiated connective tissue dysplasia as a key factor in
pathogenesis of maxillofacial disorders in children and adolescents. Archiv
EuroMedica.
2020. Vol. 10; 2: 83-94. https://dx.doi.org/10.35630/2199-885X/2020/10/2.24
- Ivanyuta
O.P., Al-Harasi G. Modification
of the dental arch shape using graphic reproduction method and its
clinical effectiveness in patients with occlusion anomalies // Archiv
EuroMedica.
2020. Vol. 10; 4: 181-190. https://dx.doi.org/10.35630/2199-885X/2020/10/4.42
- Ivanov
S.Yu., Lepilin A.V. Morphological specifics of craniofacial complex in people with
varioustypes of facial skeleton growth in case of transversal
occlusion anomalie. Archiv
EuroMedica.
2019. Vol. 9; 2: 5-16. https://doi.org/10.35630/2199-885X/2019/9/2/5
- Kochkonyan
T.S., Al-Harazi G. Clinical types of hard palatal vault in people with various gnathic
dental arches within physiologically optimal norm. Archiv
EuroMedica.
2022. Vol. 12; 1: 91-98. https://dx.doi.org/10.35630/2199-885X/2022/12/1.20
- Kochkonyan
T.S., Al-Harazi G. Specific features of variant anatomy and morphometric
characteristics of the palatal vault in adults with different
gnathic and dental types of arches. Archiv
EuroMedica.
2021. Vol. 11; 3: 54-60. https://dx.doi.org/10.35630/2199-885X/2021/11/3/14
- Kochkonyan
T.S., Al-Harazi G. Morphometric patterns of maxillary apical base variability in people
with various dental arches at physiological. Archiv
EuroMedica.
2021. Vol. 11; 4: 123-129. https://dx.doi.org/10.35630/2199-885X/2021/11/4.29
- Kochkonyan
T.S., Shkarin V.V., Dmitrienko
S.V.
Morphological
features of dental arch shape and size within baby teeth bite
period. Archiv
EuroMedica.
2022. 12; 3: e1. DOI 10.35630/2022/12/3.23
- Kochkonyan
T.S., Shkarin V.V. Variant anatomy of transitional occlusion dental arch at optimal
occlusal relationships. Archiv
EuroMedica.
2022. Vol. 12; 2: 128-133. https://dx.doi.org/10.35630/2199-885X/2022/12/2.32
- Kondratyeva
T. Methodological approaches to dental arch morphology studying. Archiv
EuroMedica.
2020. Vol. 10; 2: 95-100. https://dx.doi.org/10.35630/2199-885X/2020/10/2.25
- Korobkeev
A. A. Anatomical and topographical features of temporomandibular joints in
various types of mandibular arches. Medical
News of North Caucasus.
2019;14(2):363-367. DOI: http://dx.doi.org/10.14300/mnnc.2019.14089
(In Russ.).
- Korobkeev А.A. Anatomical features of the interdependence of the basic parameters
of the dental arches of the upper and lower jaws of man. Medical
news of North Caucasus.
2018. – Vol. 13. – № 1-1. – P. 66-69. (In Russ., English
abstract). DOI – https://doi.org/10.14300/mnnc.2018.13019
- Korobkeev
A. A. Variability of odontometric indices in the aspect of sexual
dimorphism. Medical
News of North Caucasus.
2019;14(1.1):103-107. DOI –
https://doi.org/10.14300/mnnc.2019.14062 (In Russ.).
- Lepilin
A.V. A
biometric approach to diagnosis and management of morphological
changes in the dental structure.
Archiv EuroMedica. 2020. Vol. 10; 3: 118-126. https://dx.doi.org/10.35630/2199-885X/2020/10/3.30
- Lepilin
А.V., Puzdyrova M.N., Subbotin R.S. Dependence of stress strain of dental hard tissues and periodontal
on horizontal deformation degree. Archiv
EuroMedica.
2019. Vol. 9; 1: 173-174. https://doi.org/10.35630/2199-885X/2019/9/1/173
- Lepilin
А.V., Fomin I.V., Budaychiev G.M. Improving
odontometric diagnostics at jaw stone model examination. Archiv EuroMedica.
2018. Vol. 8; 1: 34-35. https://doi.org/10.35630/2199-885X/2018/8/1/34
- Mazharov
V. N. Peculiarities of the orientation of the occlusion plane in people
with different types of the gnathic part of the face. Medical
News of North Caucasus.
2021;16(1):42-46. DOI – https://doi.org/10.14300/mnnc.2021.16011
(In Russ.)
- McNamara
J.A. Orthodontic and Dentofacial Orthopedics. Needfarm Press. Inc., 1998.
555 p.
- McLaughlin
R. P., Bennett J. C., Trevisi H. J. Systemized orthodontic treatment mechanics. – Elsevier Health
Sciences, 2001. – 324 р.
- Nanda
R. Esthetics and biomechanics in orthodontics [Text] / R. Nanda. –
Oxford University Press in the UK: CRC Press.– 2015 – 612 р.
– ISBN: 978-1-4557-5085-6
- Nelson
S.J. Wheelerʼs dental anatomy, physiology, and occlusion [Text] / S.J.
Nelson. – London: Second Edition. – 2015 – 350 s. – ISBN:
978-0-323-26323-8
- Phulari,
B.S. An atlas on cephalometric landmarks [Text] / B. S. Phulari. –
London: First Edition, 2013. – ISBN: 978-93-5090-324-7 – 213 s.
- Porfiriadis
M.P. mathematic
simulation for upper dental arch in primary teeth occlusion. Archiv euromedica,
2018. Vol. 8; 1. P. 36-37. https://doi.org/10.35630/2199-885X/2018/8/1/36
- Porfiriadis
M.P., Budaychiev G.M-A. Dentoalveolar specifics in children with cleft palate during
primary occlusion period. Archiv
EuroMedica.
2018. Vol. 8; 1: 33-34. https://doi.org/10.35630/2199-885X/2018/8/1/33
- 52. Postnikov
M.A., Chigarina S.E. Osteopathic
correction in treating patients with tension headache symptom
against TMJ dysfunction // Archiv
EuroMedica.
2021. Vol. 11; 4: 111-118. https://doi.org/10.35630/2199-885X/2021/11/4.27
- Proffit
R.W. Contemporary Orthodontics / R.W. Proffit // 6rd ed. St Louis, Mo:
Mosby, 2018. – 744 p.
- Rashmi
G.S. Textbook of Dental Anatomy, Physiology and Occlusion. 1st ed. New
Delhi: Jaypee Brothers Medical Publishers Ltd; 2014.
DOI:
10.5005 / jp / books / 11841
- Roth
R. H. Gnathological concepts and orthodontic treatment goals. Technique
and Treatment with Light Wire Appliances. 2nd ed. – St. Louis: C.
V. Mosby, 1972.
- Rufenacht
C. R. Principles
of esthetic integration. – Chicago: Quintessence Pub. Co, 2000. –
248 p.
- Slavicek,
R. The Masticatory Organ: Functions and Dysfunctions / R. Slavicek. –
Klosterneuburg: Gamma Med. Fortbildung, 2002. – 544 p.
- Suetenkov
D.E., Firsova I.V., Kubaev A. A
modified method for rapid palatal expansion anchored on
mini-implants. Archiv
EuroMedica.
2022. Vol. 12; 1: 84-90. https://dx.doi.org/10.35630/2199-885X/2022/12/1.19
- Shkarin
V.V., Grinin V.M., Khalfin R.A.
Specific features of central point location between incisors in
people with physiological occlusions // Archiv
EuroMedica.
2019. Vol. 9; 2: 165-167. https://doi.org/10.35630/2199-885X/2019/9/2/165
- Shkarin
V.V., Grinin V.M., Khalfin R.A. Specific features of joint space in patients with physiological
occlusion on computed tomogram head image // Archiv
EuroMedica.
2019. Vol. 9; 2: 182-183. https://doi.org/10.35630/2199-885X/2019/9/2/182
- Tefova
K., Dmitrienko T., Kondratyeva T. Modern
x-ray diagnostics potential in studying morphological features of
the temporal bone mandibular fossa. Archiv
EuroMedica.
2020. Vol.
10; 1. Р.
118-127. https://doi.org/10.35630/2199-885X/2020/10/36
- Weisheim
L.D., Melekhow S.V. Analytical approach within cephalometric studies assessment in
people with various somatotypes. Archiv
EuroMedica.
2019. Vol. 9; 3: 103-111. https://doi.org/10.35630/2199-885X/2019/9/3.29
back
