- Home
- About the Journal
- Peer Review
- Editorial Board
- For Authors
- Reviewer Recognition
- Archive
- Contact
- Impressum
- EWG e.V.
The high prevalence of dental diseases among different contingents of young people (conscripts, students of colleges and universities, including students from abroad) has no tendency to decrease. Young people with high prevalence of dental anomalies tend to disorders of the functions of the dental system, aesthetic changes and the formation of a psychoemotional complex. The conducted research establishes the need for the treatment of dental anomalies in young people.
Keywords: prevalence of dental anomalies and deformities, need for orthodontic treatment
Dental anomalies are disproportions in the development of the jaws, disorders of the dentition and anomalies of the teeth [42]. Dental anomalies are one of the main dental diseases characterized by high prevalence.
According to WHO, the anomalies of the disproportion of the development of the jaws include macrognathia, micrognathia of the upper, lower or both jaws; prognathia, retrognathia and asymmetry of the position of the jaws are belong to the anomalies of the position of the jaws relative to the base of the skull. The anomalies of dentition include distal occlusion, mesial occlusion, excessive overlap (horizontal overlapping bite, vertical overlapping bite, open bite, cross bite of the lateral teeth), lingual occlusion of the lateral teeth of the lower jaw, etc. The anomalies of the teeth include crowding, displacement, rotation, spaces between teeth, transposition.
There are several research articles about the prevalence of dental anomalies in children and teenagers. However, there was also insufficient structured information on the prevalence of dental anomalies in young people and adults [42].
The results of the research by Simakova A.A. et al. revealed that there is a high prevalence of dental anomalies in the adult population and a relatively few publications on this topic that requires the further researches of dental anomalies, monitoring of the situation, development of prevention programs and their implementation [42].
Data on the prevalence of dental anomalies in adults help to assess the level of orthodontic pathology, indicators in dynamics. It will also help to draw up programs for the prevention and treatment of orthodontic pathologies [42].
A dental examination of 18 to19-year-olds conducted in 2001 in Arkhangelsk (Russia) revealed a high prevalence of dental anomalies (72,3±3,2%) [42].
Makeeva I.M. and co-authors identified maxillofacial deformities in 69.3% of Moscow students aged of 16 to 2- year-olds and of 21 to 25-year-olds [31].
In 1995, an examination was conducted in Yekaterinburg (Russia) revealed the following prevalence of dental anomalies: of 18 to 25 year-olds – 40.7%, of 26 to 45 year-olds – 69% [36].
An examination of 1600 patients of 12 to 44-year-olds in Khabarovsk (Russia) revealed the following prevalence of dental anomalies: it was 58,3% in the 18-year-old group and 58,5% in the 35-44-year-old group [43].
The index of orthodontic treatment need is used to distribute the types of bite according to the level of need for orthodontic treatment to assess the individual patients and population groups [12, 21]. These indicators were created to minimize subjectivity. The subjectivity complicates the assessment of bite and diagnosis. The indicators are multifunctional and can be used to evaluate the results of orthodontic treatment [40].
Occlusive indices are often used worldwide for the purpose of epidemiological assessment of the need for orthodontic treatment. It helps to prioritize orthodontic services [8, 10, 23, 48, 50].
Epidemiological studies worldwide indicate a high need for orthodontic treatment. Thus, J. M. AlmerichSilla et al. (2014) found that 20% of the residents of Valencia (Spain) need orthodontic treatment [4]. According to D. Damle et al. (2014) 23.6% of the population of Haryana (India) have dental anomalies and deformities and need their correction [13]. Al Jeshi et al. (2014) established the need for orthodontic treatment in 14.4% of residents of Dubai (UAE) [3]. According to G. Laganà et al. (2015) 17% of the Albanian population needs to correct the dental anomalies and deformities [25]. The study conducted by Ajayi E.O. (2015) in Nigeria, 21.5% of the population need to treat dental anomalies and deformities [1]. The research conducted by Atisook P. et al. (2014) in Bangkok (Thailand) 37.5% of the city's residents were found to have dental anomalies and deformities and need to treat dental anomalies and deformities [6]. According to Fundagul B. et al. (2015), 28.7% of Turkish residents need orthodontic treatment [17].
According to Richmond S. (1994), due to a deficiency of orthodontists and funding, it is imperative to provide orthodontic treatment for patients with the highest need for treatment. Thus, the quality of orthodontic treatment will be improved. Organizational issues are solved when studying the need for orthodontic treatment [2, 46].
In some cities of Russia the prevalence of dental anomalies and deformities was assessed. There is not data on the need in these cities [45, 46].
In the city of Kemerovo (Russia), 41.98% of the examined patients with dental anomalies as well as 54.87% of Kemerovo patients have the need for orthodontic treatment. [40].
According to Skubitskaya A.G. and Strusovskaya O.G. the most massive group of patients in Volgograd was the group of 18 to 35-year-olds, which was 66%. Among all age groups "Anomaly of the position of individual teeth. Crowding of teeth" was the most common diagnosis which amounted to 88,58% [44].
The lowest level of the frequency of dental anomalies and deformities is characterized by the period of replacement bite [33]. According to A.G. Arzumanyan the prevalence of maxillary anomalies and deformities in Troitsk and Novomoskovsk Autonomous Regions of Moscow is 76.5%.
The Dental Aesthetic Index (DAI), the Index of Orthodontic Treatment Need (IOTN) and the ICON index of complexity outcome and need for orthodontic treatment are used to determine the need for orthodontic treatment in patients [39, 41, 47].
According to M.V. Sergeeva (2022) a study of 18-year-old residents of Kuzbass (Russia) revealed the prevalence of dental anomalies equal to 75,1% . 13,8% of them were anomalies of individual teeth, 14,4% were anomalies of dentition in the transversal direction, 22,9% were anomalies of the ratio of dentition in the sagittal direction, in 68,3% of cases combined dental anomalies were recorded [40]. Using the ICON index, it was revealed that 32,6% of the examined patients were indicated for treatment (12,7%) or selective treatment (19.9%). 67,5% of examined patients had acceptable occlusion pathologies. Using the IOTN index, high (26,5%), very high (1,2%), average (24,1%) and low (35,5%) need for treatment was revealed in 87,3% of the surveyed people aged 18 years. According to the DAI index, the need for treatment is average (80,6%), high (15,35%), very high (3,0%) in 98,95% of the examined 18 year old patients. Caucasoid and Mongoloid races have important differences (p=0,337) [40].
Comparing the current data on the prevalence of dental anomalies and deformities with the data of an epidemiological study conducted in the 80-90s of the last century [18, 26, 37] we can conclude that the prevalence has remained high for several decades, and in some regions, the steady growth of this indicator.
The results of the clinical examination by E.S. Gileva (2007), objectified by the DAI index (23.48 ± 1.25 points), indicate a high prevalence of dental anomalies in young people, with the dominance of occlusion anomalies (34,8%) and the crowded position of the frontal group of teeth (33,1%). Minor easily corrected aesthetic disorders were more often detected (81,9 %), severe socially unacceptable forms of dental anomalies (DAI > 36 points) were diagnosed in 2,8% of individuals [19].
The prevalence of dentoalveolar anomalies among students in Moscow, according to I.M. Makeeva, amounted to 69,3%. Anomalies of occlusion occurred in 35%. Among them are distal and mesial occlusion (in 8,5 and 10%, respectively), vertical incisal disocclusion (3,2%), and cross occlusion (5,5%). DAI index values <25 were determined in 68% of the examined, DAI values equal to 26-30 - in 16% of young people, DAI values equal to 31-35 - in 11%. Values of the DAI index >36, indicating the presence of very severe disorders and an unconditional need for treatment, were found in 5% of the examined [30].
The epidemiological study of adolescents and adults in the Far East of Russia conducted by Y.M.Glukhova (2010) revealed a high incidence of anomalies, which amounted to 58,84% ± 1,38%. The need for orthodontic treatment is 47,59%, according to the DAI, and, in accordance with the IOTN, reaches 39,17% (p ≤ 0,05) [20].
The assessment of the need for orthodontic treatment according to the IOTN index, conducted by Wang G et al., in Hong Kong schoolchildren, indicates that 12% do not require orthodontic treatment (Grade 1), 18% had minor neediness (Grade 2), 33% had an average degree of neediness (Grade 3), 33% - high (Grade 4), and 4% - a very high degree of need (Grade 5) [49].
When studying of the crowding of incisors in patients aged 15 to 50 years living in the USA who have not undergone orthodontic treatment, the following prevalence was revealed: 50,0% of them have a mild crowding of incisors or do not have at all, 23,0% – moderate crowding, 17,0% - severe crowding of incisors (Buschang P.H., Shulman J.D., 2003) [11].
The presented results of epidemiological surveys in Russia and abroad confirm the data on the high prevalence of dental anomalies and deformities in young people. The analysis of the literature data at the same time indicates that there is no tendency to decrease the frequency of dental anomalies over the past decades.
A comprehensive dental examination of 1,398 students of Bashkir State Medical University aged 18 to 25 years including 372 male and 1,026 female was conducted at the Department of Dentofacial Orthopedics of the University.
Dental anomalies were assessed according to the classification of the Department of Orthodontics and Pediatric Prosthetics of the Moscow State Medical University (1990) and ICD-10. The data was documented in the medical record of each subject.
The need for orthodontic treatment was determined using the DHC dental status component of the IOTN Index of Orthodontic Treatment Need (Evans R., Shaw W.C., 1987) [14] is based on the index used by the Swedish Dental Committee and is designed to reflect those occlusive features that may affect the preservation and functioning of the dentition.
To do this, one of the worst signs of malocclusion is described and attributed to one of five degrees reflecting the need for orthodontic treatment: 1 degree — no need; 2 degree — little need; 3 degree — moderate need; 4 degree — great need; 5 degree — very great need
Index of Orthodontic Treatment Need:
5.i. Impeded eruption of teeth (except for third molars) due to crowding, displacement, the presence of supernumerary teeth, retained deciduous teeth and any pathological cause.
5h. Extensive hypodontia with restorative implications (more than 1tooth missing in any quadrant) requiring pre-restorative orthodontics.
5.a. Increased overjet greater than 9mm.
5.m. Reverse overjet greater than 3,5min with reported masticatory and speech difficulties.
5.p. Defects of cleft lip and palate and other craniofacial anomalies.
5.s. Submerged deciduous teeth.
4.h. Less extensive hypodontia requiring prerestorative orthodontics or orthodontic space closure to obviate the need for a prosthesis.
4.a. Increased overjet greater than 6mm but less than or equal to 9mm.
4.b. Reverse overjet greater than 3,5mm with no masticatory or speech difficulties.
4.m. Reverse overjet greater than 1mm but less than 3,5mm with recorded masticatory and speech difficulties.
4.c. Anterior or posterior crossbites with greater than 2mm discrepancy between retruded contact position and intercuspal position.
4.1. Posterior lingual crossbite with no functional occlusal contact in one or both buccal segments.
4.d. Severe contact point displacements greater than 4mm.
4.e. Extreme lateral or anterior open bites greater than 4mm.
4.f. Increased and complete overbite with gingival or palatal trauma.
4.t. Partially erupted teeth, tipped and impacted against adjacent teeth.
3.a. Increased overjet greater than 3,5 mm but less than or equal to 6 mm with incompetent lips.
3.b. Reverse overjet greater than 1 mm but than or equal to 3,5 mm.
3.c. Anterior or posterior crossbite with greater than 1 mm but less than or equal to 2 mm discrepancy between retruded contact position and intercuspal position.
3.d. Contact point displacements greater than 2 mm but less than or equal to 4 mm.
3.e. Lateral or anterior open bite greater than 2 mm but less than or equal to 4 mm.
3.f. Deep overbite complete on gingival or palatal tissues but no trauma.
2.a. Increased overjet greater than 3.5mm but less than or equal to 6mm with competent lips.
2.b. Reverse overjet greater than 0mm but less than or equal to 1mm.
2.c. Anterior or posterior crossbite with less than or equal to 1mm discrepancy between retruded contact position and intercuspal position.
2.d. Contact point displacements greater than 1mm but less than or equal to 2mm.
2.e. Anterior or posterior open bite greater than 1mm but less than or equal to 2mm
2.f. Increased overbite greater than or equal 3.5mm without gingival contact.
2.g. Pre-normal or post-normal occlusions with no other anomalies (includes up to half a unit discrepancy).
1. Extremely minor maloccusions including contact point displacements less than 1 mm.
The DAI - Dental Aesthetic Index, proposed in 1986 at the Medical College of the University of Iowa, was used to assess the state of the dental system by the prevalence and severity of dental anomalies. The standard DAI is calculated using regression, when the measured values are multiplied by regression coefficients, and the resulting numbers are added to the constant of the regression equation. The regression equation for calculating the standard DAI is as follows:
(missing teeth × 6) + (crowding) + (space between teeth) + (diastema ×3) + (largest anterior deviation on the upper jaw) + (largest anterior deviation on the lower jaw) + (anterior maxillary overlap ×2) + (anterior mandibular overlap ×3) + (vertical anterior space ×4) + (anterior-posterior ratio of molars ×3) +13.
An index value of less than 25 indicates the absence of pathology or minor disorders. The need for treatment in this case is small or it is not required at all. DAI values in the range of 26-30 indicate obvious malocclusion, which requires selective treatment. The values of DAI 31-35 indicate severe malocclusion, and the need for treatment is desirable. Index values above 36 indicate very severe malocclusion, and treatment in this case is mandatory.
Statistical processing was conducted using standard methods of mathematical statistics in Microsoft Excel and the Statistica for Windows 10.0 software package. The Student's criterion for assessing the significance of the difference in statistical coefficients using average errors, arithmetic mean (M), standard error of the mean (m), standard deviation (δ), reliability criterion (t) were calculated.
The prevalence of dentoalveolar anomalies in the examined patients was high and amounted to 83.12 ± 1.0%. The prevalence of dentoalveolar anomalies was considered depending on gender and was in 82.26±1.98% in men and in 83.43±1.16% in women.
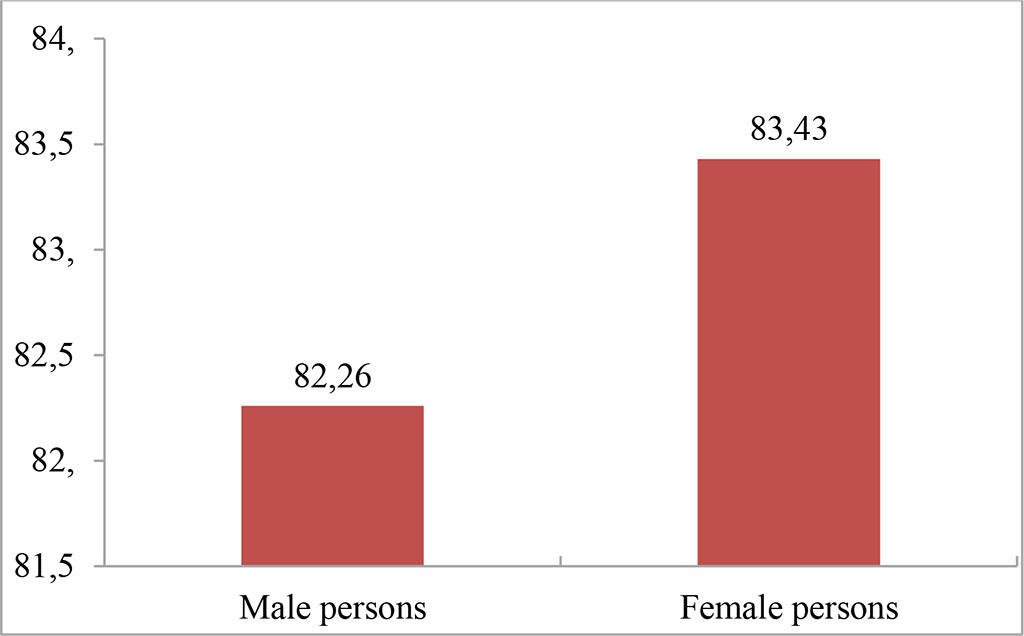
Figure 1. The prevalence of dental anomalies in young people by gender
The prevalence of dental anomalies was examined for various types of anomalies. Combined anomalies predominate in the structure of dentoalveolar anomalies (65.23 ± 1.4%). Anomalies of dentition were detected in 22.72 ± 1.23%, anomalies of occlusion – 6.54± 0.72%, anomalies of teeth – 5.51± 0.67%. The structure of dentoalveolar anomalies, separately by gender, is as follows: anomalies of teeth were diagnosed in 3.77 ± 1.09% of men and in 4.87± 0.74% of women, anomalies of dentition in 22.04± 2.37% of men and in 17.74± 1.31% of women, anomalies of occlusion were observed in 4.84± 1.23% of males and in 5.65±0.79% of female, combined anomalies were registered in 51.61±2.86% of men and in 55.17±1.7% of women. Distal occlusion was more common among occlusion anomalies (49.31±5.73%). Deep incisor occlusion was in second place – 21.93±4.75%. Vertical incisor dysocclusion was detected less frequently (15.07±4.1%). According to the frequency of occlusion anomalies, cross occlusion was in fourth place (10.96±3.58%).
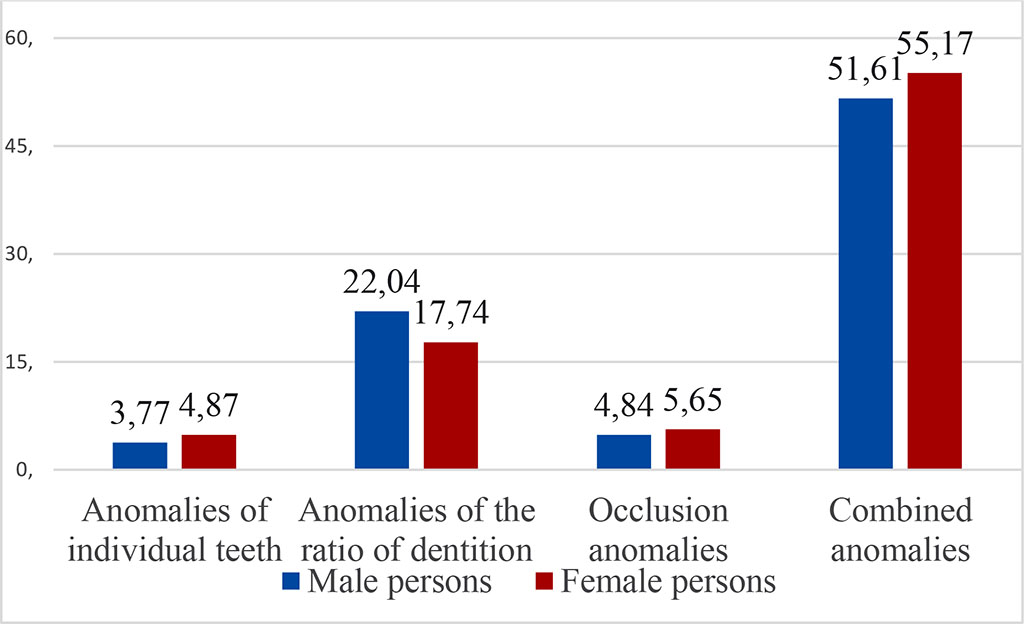
Figure 2. The structure of dentoalveolar anomalies
The results of the assessment of the state of occlusion using the DAI index are as follows: the indicators of the aesthetic index DAI below 25 which was interpreted as indicating the presence of minimal malocclusion, were determined in 78.54 ± 1.1% of the examined. DAI values equal to 26-30 are interpreted as a clear malocclusion, as a result of which selective treatment is necessary, were detected in 13.73± 0.92%. According to the results of the research, DAI values from 31 to 35, characteristic of severe malocclusion, occur in 4.86 ± 0.57% of young people. Indicators of the aesthetic index from 36 and above, determining the presence of very severe malocclusion and requiring mandatory treatment, were observed in 2.86± 0.45%.
Table 1. DAI Aesthetic Index values
| DAI value | Male persons, % | Female persons, % |
| DAI <25 | 76,34±2,2 | 79,34±1,26 |
| DAI 26-30 | 15,05±1,85 | 13,25±1,06 |
| DAI 31-35 | 6,99±1,32 | 4,09±0,62 |
| DAI >36 | 1,61±0,65 | 3,31±0,56 |
There is a strong dependence in the distribution of DAI index values – the higher the index value, the rarer it is (Fig. 3).
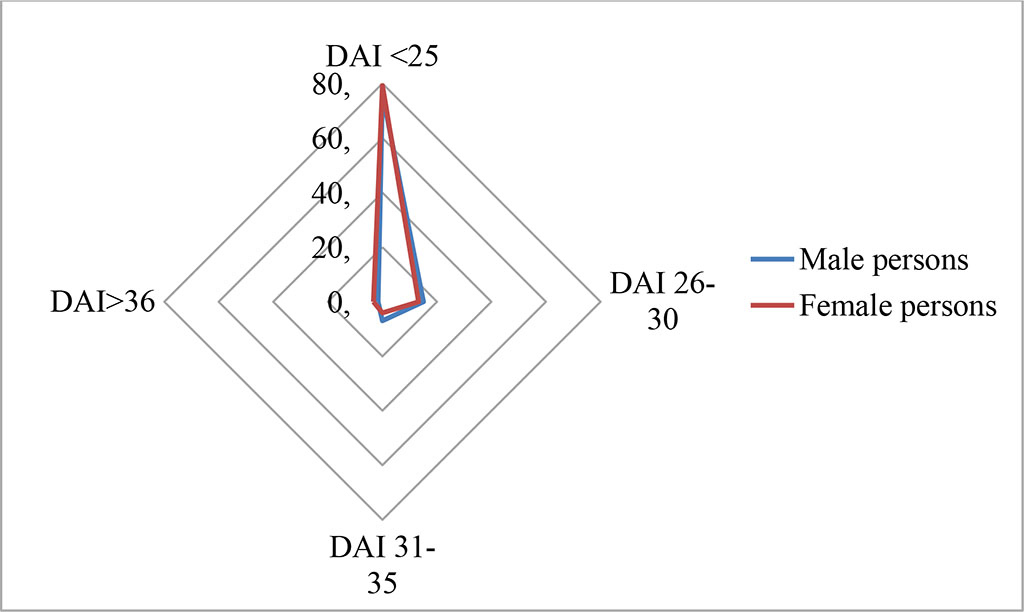
Figure 3. DAI Index values
According to the interpretation of the component indicators, the DHC of the IOTN index is 31.69±1.24% of the examined patients need treatment (Grade 1), 44.85±1.33% have a low need (Grade 2), for 15.74±0.97% of individuals the average/borderline degree of need was determined (Grade 3). 6.58±0.66% of the examined have a high need (Grade 4), and only for 1.14± 0.28% there is a very high need for orthodontic treatment (grade 5), which is consistent with the data of foreign researchers (1,2,3,4,5,6,7) (Table 1)
According to the interpretation of the component indicators of the DHC of the IOTN index is 31.69±1.24% of the examined patients need orthodontic treatment (Class 1), 44.85±1.33% have a low need (Class 2), for 15.74±0.97% of individuals the average/borderline degree of need was determined (Class 3). 6.58±0.66% of the examined have a high need (Class 4), and only 1.14± 0.28% of patients have a very high need for orthodontic treatment (Class 5) (Table 2).
Table 2. Class distribution of the DHC component of the IOTN index
| IOTN class | Male persons, % | Female persons, % |
| 1 class | 32,53±2,43 | 31,38±1,45 |
| 2 class | 43,28±2,57 | 45,42±1,55 |
| 3 class | 16,67±1,93 | 15,4±1,13 |
| 4 class | 6,99±1,32 | 6,43±0,77 |
| 5 class | 0,54±0,38 | 1,36±0,36 |
Thus, the results of the examinations indicate a high prevalence of dental anomalies in young people (83.12 ± 1.0%). At the same time, according to the interpretation of the aesthetic dental index DAI, 78.54 ± 1.1% of the examined have minimal disorders and require selective treatment or do not require it at all. An analysis of the results of the assessment of dental anomalies by the DHC component of the IOTN index showed that 68.31 ± 1.2% need an orthodontic treatment.

|
||