- Home
- About the Journal
- Peer Review
- Editorial Board
- For Authors
- Reviewer Recognition
- Archive
- Contact
- Impressum
- EWG e.V.
Cite as: Archiv EuroMedica. 2022. 12; 3: e1. DOI 10.35630/2199-885X/2022/12/3.23
The study of morphometric characteristics of baby teeth bite dental arches presents an urgent issue for morphology and pediatric dentistry. To identify the morphological features of the baby teeth bite, dental arch biometrics was done involving children aged 3-5, while following the recommendations from the Ethics Committee. The measurements relied on baby teeth odontometry, with the length of the dental arches, their transversal and diagonal dimensions identified, all this followed by the construction of diagnostic triangles. The study showed the rate between the dental arch width with the length, the width sum of the 10 baby teeth crowns and the magnitude of the systemic component. The data obtained through the study served to determine the rate between the dental arch diagonals and the odontometric indicators, as well as enabled to identify the value of the dental-diagonal coefficient, which is 1.01±0.01 for the upper arch and 1.02±0.01 for the lower jaw dental arch.
Keywords: morphometry, odontometry, plaster model biometry, baby teeth bite.
Within the baby teeth bite period, the shape and size of the dental arches have their own features, which differ from the dental permanent bite. The gaps (diastemas, primate tremas, etc.) between certain teeth in the baby bite does not allow identifying the length of the dental arch based on the total component of the dental crown widths, as is done conventionally when studying patients with a fully-developed permanent bite [1,5,7]. Mathematical and graphical constructions of dental arches, which relied on odontometric indicators in the permanent teeth bite period, allowed identifying the arcade and dental components of the dental arch types, while taking into account advanced classifications and sexual dimorphism [4,13,20,27].
Aiming to preserve the optimal individual shape of the baby teeth bite dental arch, therapeutic and preventive prosthetics methods were proposed that focused on maintaining the height of the bite and the place in the dental arch following premature removal of baby teeth in various groups of patients [3,24]. During that, premature removal of baby teeth, especially in the chewing segment, was noted to contribute to a decrease in facial gnathic part height as well as pathological changes in the mandibular joint [8,11,19]. As it has been shown, the treatment of dental arch deformities developing after tooth extraction is accompanied by changes affecting the periodontal complex, and is often hard and time-consuming [6,12,21,26].
The methods employed to study dental arches within periods of temporary and replacement bites are few and even sometimes contradictory, which explains the relevance of this study [22,23,25]. The A.M. Schwarz technique that is proposed within this study and which is based on the graphical structure of an arc appearing like a semicircle with a diameter matching the molar distance measured between the vestibular-distal points of the second baby molars, has already become classics whereas its details are to be found in special academic literature [2,10]. However, when analyzing this technique, no transversal dimensions of different dental arches and their correlation with the teeth size or other basic parameters of dental arches were revealed. As for the period of transitional and permanent bite, the available studies focus on the diagonal dimensions of the dental arches and present their features in various types of dental systems. There is also interrelationships of diagonal dimensions with odontometric indicators and the calculation of dental-diagonal indices for upper and lower jaw dental arches shown [17]. However, the data of jaw plaster model biometric examination serve the main diagnostic parameters when identifying issues affecting the shape and the size of dental arches, as well as they are also used a criterion when choosing treatment options and identifying the effectiveness of the respective option [9,14-16,18].
The available literature, though, offered us no data on similar research carried out through baby teeth bite, and all of the above explains the aim of this study.
Aim of study: to carry out a biometric study and to identify the main morphometric parameters of dental arches while assessing their features through the of baby teeth bite period.
The study focused on the main parameters of dental arches, while involving 32 children falling within the age group that belongs to the baby teeth bite period (3-5 y.o.). The ratio of the dental arches and occlusal relationships matched the age norm (Fig.1).

Figure 1 – Оcclusal characteristics in participants with optimal functional occlusal norm
Biometric analysis of the dental arches main parameters was carried out both directly in the oral cavity and on jaw plaster models. The marks for measuring were the points located on the teeth crowns vestibular surfaces near their occlusal surfaces and the cutting edge (Fig. 2).#
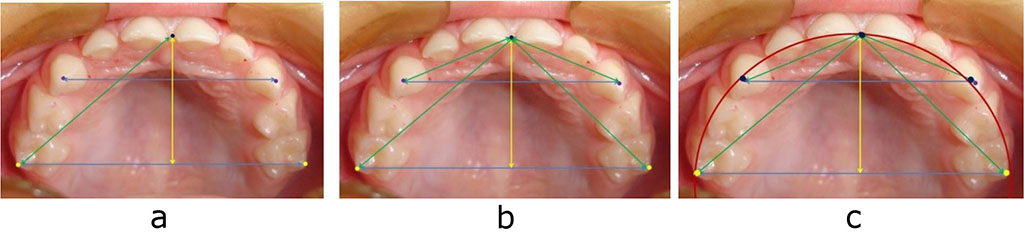
Figure 2 – Major reference marks for measuring baby bite dental arches (a), geometric construction of diagnostic triangles (b) and graphic reproduction (c)
The biometric analysis relied on identifying odontometric indicators, while special attention was paid to the mesial-distal diameters of the baby teeth crowns that make up the dentition and affect the dental arch shape. The obtained data allowed identifying the total size for all the teeth, as well as for the anterior set (incisors and canines) in particular, which many researchers place focus on.
The total width of the teeth crowns is the basis for detecting the dental system type, while also allowing us to assess the match with the odontometric indicators of antagonists.
Given the natural gaps between baby bite teeth, we conducted a comparative analysis matching the total size of the teeth with the length of the dental arch following H.N. Nance (1947). In this case, a flexible (ligature) wire (thread) was used to be placed on the dental arch near the vestibular and occlusal surface (cutting edges) border, from the second molar’s vestibular-distal point to the antimere identical mark. The length of the wire was measured to match it against the size of the teeth. Transversal dimensions were identified between the second molars (the dental arch width) and between the canines (the anterior arch width), with the tearing tubercles of the baby canines serving as references.
The incisor point, which was the dental arch center, served as a reference point for identifying the sagittal dimensions of the dental arch and its anterior section, while also allowed measuring the diagonal dimensions of the arch and that of the anterior section.
The construction of diagnostic triangles began from the base, whose value corresponded to the dental arch molar width. From its middle and running perpendicular to it, a median sagittal vertical was drawn with a distance indicated on it that matched the dental arch depth. A segment equal to the anterior arch depth was built from the resulting central point. Perpendicular to the conditional median vertical of the arch, a straight line matching the anterior section width (canine transversal distance) was laid on both sides from the depth point of the anterior section. The sides of the isosceles triangle of the anterior section matched the incisor-canine diagonal size.
The graphical construction of the arch was based on the method by A.M. Schwarz, with the diameter of the semicircle passing through the second baby molars points, and matched the dental arch width.
The obtained linear reference marks allowed identifying the arch arcade index as the ratio of the arch width to the sum of its diagonals.
The statistical processing of the obtained data was performed with Microsoft Excel 2013 software as well as the SPSS Statistics (Version 22) statistical software package. The critical level of a possible null statistical hypothesis was set at 0.05.
The biometric study of the baby bite dental arches in children aged 3-5, allowed detecting certain features and patterns for both odontometric and linear indicators, which can be seen in Table 1.
Table 1 – Dental arch sizes in children, baby bite period (mm) (M ±m) (p ≤ 0.05)
| Odontometric and arcade parameters of dental arches | Dental arch size on jaw | |
| upper | lower | |
| Sum of 10 baby teeth crown widths | 65.25±2.09 | 61.01±2.05 |
| Dental arch width between molars | 47.85±1.85 | 43.39±1.27 |
| Dental arch length | 75.11±1.34 | 71.37±1.27 |
| Dental arch depth | 23.92±1.26 | 21.73±1.17 |
| Dental arch diagonal | 33.83±1.57 | 31.42±1.49 |
| Sum of 6 front teeth crown widths | 34.97±1.77 | 27.31±1.25 |
| Dental arch width between canines | 29.61±1.98 | 24.94±1.72 |
| Front dental arch length | 36.62±1.86 | 28.03±1.74 |
| Front dental arch depth | 7.03±0.29 | 4.79±0.27 |
| Front dental arch diagonal | 16.39±1.02 | 13.36±0.96 |
Basically, all the parameters of the upper dental arches exceeded the parameters of the antagonist one. Notable is the comparison of the dental arch length with the totality of the mesial-distal dimensions of the teeth crowns. On the upper jaw, for instance, the arch length was 75.11 = 1.34 mm, while the sum of the crown widths for 10 baby teeth was 65.25 = 2.09 mm. During that, the difference between these values was 9.86 = 0.98 mm, which is quite natural and can be accounted for by the gaps (diastemes) between baby teeth. This value can be employed as a diastema component of the baby bite upper dental arch. As far as the lower jaw is concerned, the diastemic component value was 10.36±1.03 mm, and corresponded to the difference between the arch length (71.37±1.27 mm) and the total value of the crowns of the teeth making up the baby (temporary) dentition (61.01±2.05 mm).
The sum of the dental arch diagonal dimensions on the upper jaw was an average of 67.66±1.89 mm (33.83±1.57 mm on each side) and did not reveal any significant difference from the indicators of the 10 baby teeth sum total. Yet, the value of the (arcade-diagonal) dental-diagonal index for the upper dental arch was an average of 1.01±0.009 and allowed making forecast regarding the size of the diagonals relying on the sum of the molar teeth width. On the lower jaw, the similar index value was 1.02 ± 0.01.
The dental arch depth on both jaws was, on average, half the size of the molar transversal distance, which is quite natural and can be explained by the patterns and assumptions proposed by A.M. Schwarz concerning the shape of the dental arch viewed as a semicircle with a diameter matching the inter-molar distance.
When analyzing the anterior dental arch (which was measured from the tearing tubercles of the canines), the identified patterns were similar to those observed while studying the complete arch of the baby bite. The length of the dental arches exceeded the total width of the 6 front teeth crowns by an average of 1.64±0.21 mm due to the gaps, which were most pronounced between the canine and lateral incisor (primate tremas). On the lower dental arch, the anterior section length was less than the sum of the width of the 6 front teeth crowns (1.56 ± 0.17 mm on average), which is due to the fact that the largest gap was to be seen between the molar canine and the first molar, which in turn is specific of dental arches in children featuring a proper functional age norm of baby bite. The linear parameters of the anterior arch allowed them to be used for constructing diagnostic triangles of the anterior arch, which can find its application in clinical orthodontics in order to detect issues affecting dental arches and the front teeth position.

|
||