- Home
- About the Journal
- Peer Review
- Editorial Board
- For Authors
- Reviewer Recognition
- Archive
- Contact
- Impressum
- EWG e.V.
Cite as: Archiv EuroMedica. 2024. 14; 2: e1. DOI 10.35630/2024/14/2.210
The article describes a clinical case of a combined course of dermatoses with damage to the scalp, such as psoriasis and follicular lichen planus (LPP), proceeding like pityriasis amiantacea (PA), with the formation of a severe form of cicatricial alopecia. Clinical patterns of damage to the scalp in these diseases are presented, confirming the possibility of developing cicatricial forms of hair loss, the treatment method is described.
This clinical case demonstrates the need to conduct a histological examination in patients with scarring hair loss in order to select the most effective treatment method. The variety of forms of cicatricial alopecia and their common clinical manifestations create difficulties in differential terms and require an integrated approach to their diagnosis. Proper control of inflammation can prevent the progression of cicatricial alopecia.
Keywords: cicatricial alopecia, psoriasis, lichen planus, Pityriasis amiantacea (PA), clinical picture, treatment
Scarring alopecia is the irreversible destruction of hair follicles due to inflammation or an accident. A feature of all forms of cicatricial hair loss is the irreversible death of hair follicles due to their replacement with connective tissue, which is clinically manifested by the loss of skin pattern, and pathohistologically - complete destruction of the pilosebaceous complex. Cicatricial alopecia is the end result of diseases with different etiopathogenesis and clinical picture. A large area of scarring hair loss may be a sign of severe forms of dermatosis or multiple forms at the same time. Combined pathologies of the scalp are the most difficult problem in trichology. This phenomenon is often based on comorbidity - a condition associated with the presence of several diseases in a patient, united by a common pathogenesis, which can initially complicate the diagnosis and requires histological confirmation [4,11].
Depending on the nature of the disease underlying the inflammatory reaction, the death of the hair follicle occurs primarily due to a follicle-centric process or secondary to influences external to the follicle, where it is damaged together with other skin structures. The follicular form of lichen planus is the most common cause of primary cicatricial alopecia, cicatricial alopecia in the setting of psoriasis of the scalp is classified as secondary [11].
Non-scarring hair loss due to psoriasis is a common phenomenon, which is almost always reversible and is characterized by complete hair regrowth after the cessation of the inflammatory process. For a long time, there was no accurate data on the possibility of scarring hair loss in patients with psoriasis. This phenomenon was first described in 1972 by Dr. Schuster as “destructive alopecia.” Based on the results of numerous further studies, it is believed that the duration and severity of psoriasis of the scalp are factors that predispose to the development of psoriatic cicatricial alopecia [2]. In 2021, specialists from the European Academy of Dermatology and Venereology described a study in which they collected data on 156 patients at the University of Bologna polyclinic suffering from psoriasis of the scalp, and identified several variants of the course with a specific trichoscopic picture, some of which confirm the possibility of the formation of cicatricial alopecia. In this study, seven clinical patterns were identified: plaque psoriasis, which appears as classic plaques with silvery-white scales on the surface; fine-scaly psoriasis, in which there are no clearly defined plaques, the scalp is hyperemic, with many silvery-white scales; sebo-psoriasis, manifested by fatty scales against a background of erythema without pronounced infiltration; cap-type psoriasis with silvery-white scales; asbestos-like lichen in the form of yellowish scales adhered to the hair over an erythematous background and areas of scarring hair thinning; cicatricial psoriatic alopecia, in which hair thinning occurs due to an inflammatory process, manifested by erythema with silver-white scales and milky-red areas of fibrosis; pustular psoriasis of the scalp, in which, along with classic elements of psoriasis, pustular elements can also be observed. Trichoscopic signs of all clinical forms of psoriasis of the scalp are grouped dotted vessels, twisted capillary loops [3,11].
Lichen planus, when affecting the scalp (LPP), always leads to scarring hair loss. The disease in its classic course has several clinical patterns: multifocal, in which the foci of cicatricial alopecia are small and located throughout the scalp like “footprints in snow”, diffused, in which there is a loss of hair density with less pronounced foci of cicatricial alopecia and generalized erythema; follicular lichen planus with one lesion; bitemporal form with scarring hair loss in the temporal areas; post-operative, in which irreversible hair loss occurs at the sites of surgical procedures. Upon trichoscopy of all aforementioned forms, perifolicular erythema, hyperkeratosis, and white areas of fibrosis are observed [7,10,11].
These dermatoses are based on disturbances in immunometabolic processes that cause an inadequate tissue reaction under the influence of provoking factors, the leading role of cytokines in pathogenesis has been proven; the importance of foci of chronic infection and stress factors in maintaining the pathological process has also been shown [8,9,12].
Pityriasis amiantacea (PA) is a special reaction of the scalp to various inflammatory diseases. It can occur in children and adults and often appears as a layer of dense, yellow, asbestos-like scales that, when resolved, leave behind areas of temporary non-scarring or scarring hair loss. The literature describes cases of the development of asbestos-like lichen accompanied by psoriasis, seborrheic dermatitis, mycoses of the scalp, atopic dermatitis, Darier's disease, lichen planus. Or PA can be displayed as an independent condition occurring in the neck during therapy with tumor necrosis factor α inhibitors or topical application of minoxidil. Cases of combined dermatoses of the scalp, occurring like PA, are isolated descriptions [1,5,6,9,12].
The purpose of this study is to present a clinical case of a patient with severe cicatricial alopecia.
A 40-year-old female patient admitted to a dermatovenerologist with complaints of hair loss, itching and burning of the scalp, and skin rashes. She got sick a few years ago after stress, when she first noticed patches of hair thinning that slowly increased, then rashes appeared on the elbows and on the back of the head.
Objectively: on the scalp, in the crown area with transition to the temples, large foci of cicatricial alopecia, irregularly shaped, prone to peripheral growth and fusion, with layered yellow scales on the surface were observed (Fig. 1). On the back of the head there were psoriatic plaques, also covered with layered white scales, reminiscent of asbestos, which fit tightly to the skin and envelop the tufts of hair under a white sheath (Fig. 2). The oral mucosa was without any specific rashes. On the skin of the elbows and lower extremities – singular pink-red psoriatic plaques with silver-white scales were observed, while no more rashes were observed on other parts of the body. Psoriatic triad is positive. The nail plates had transformed to resemble a thimble.

Fig. 1 Manifestations of follicular lichen planus in the frontal-parietal

Fig. 2 Psoriatic rashes in the occipital region
Upon trichoscopy of the foci of hair loss in the area of the crown and temples, perifollicular erythema and hyperkeratosis were observed, in the center - extensive, milky-red zones of fibrosis and single preserved terminal hairs. The hair shafts at the site of inflammation were enveloped in layered, dense, yellow scales (Fig. 1 a, b). In the area of the back of the head there were plaques, on the surface of which there were layered, silvery-white scales in the form of massive layers; upon trichoscopy: vessels in the form of globules, twisted capillary loops (Fig. 2 a, b). When performing a pull test, anagen hair with a preserved internal epithelial sheath was obtained.
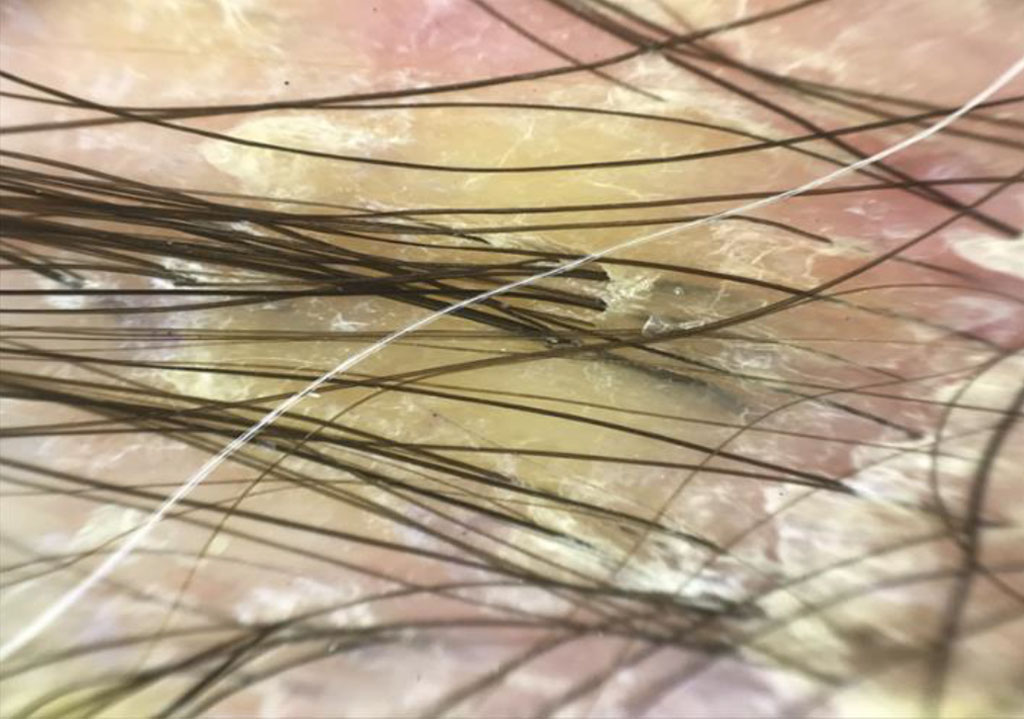
Fig. 1a Trichoscopy of follicular lichen planus: yellowish thick scales covering several hairs

Fig. 1b Trichoscopy of follicular lichen planus: erythema, follicular hyperkeratosis, milky red areas of fibrosis

Fig. 2a Trichoscopy of psoriasis: layered silvery-white scales
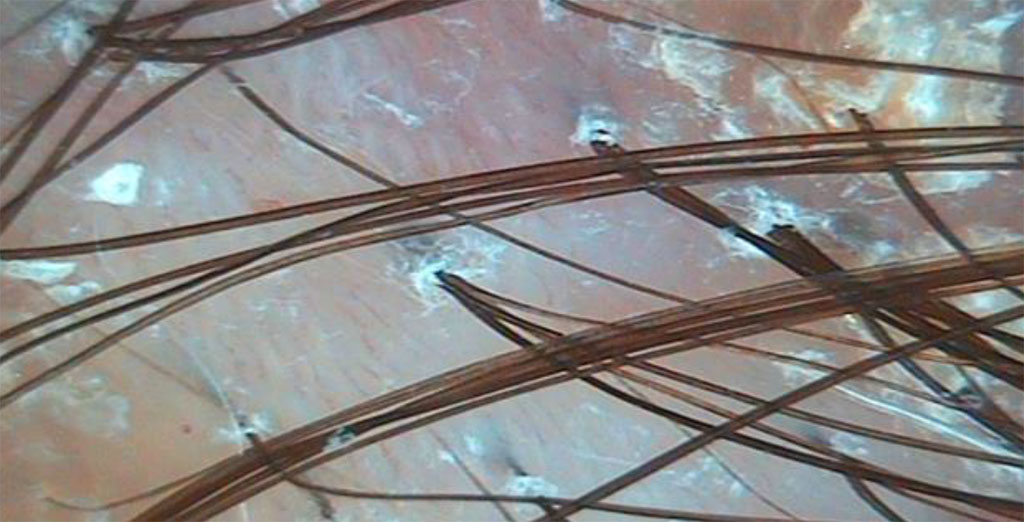
Fig. 2b Trichoscopy of psoriasis: twisted capillary loops, milky-red areas of fibrosis
Based on the clinical picture and trichoscopy data, a diagnosis was made: Psoriasis vulgaris, progressive stage. Psoriatic cicatricial alopecia. Systemic treatment with methotrexate was carried out at a dosage of 15 mg intradermally once a week, and a gel with clobetasol propionate was applied to the rash daily. During 3 months of treatment, the rashes in the elbows and shins resolved, the psoriatic plaques on the back of the head cleared, revealing areas of scarring and non-scarring hair loss, but in the area of the crown and temples, the inflammatory process persisted, and itching and hair loss keep bothering the patient.
Considering the complexity of the clinical case after discontinuing systemic treatment, a histological examination was carried out in the areas of active inflammation in the vertex. The resulting biopsy revealed 17 sections of hair, mainly in the anagen phase, with a shaft thickness of 59-64 microns, preserved histological structure of the deeper structures of the follicle, hypotrophy of the follicular epithelium and perifollicular fibrosis at the level of the infundibulum, with the formation of gaps similar to the «Max-Joseph space», mild lymphocytic infiltration, not penetrating the epithelium; the number of sebaceous glands was reduced.
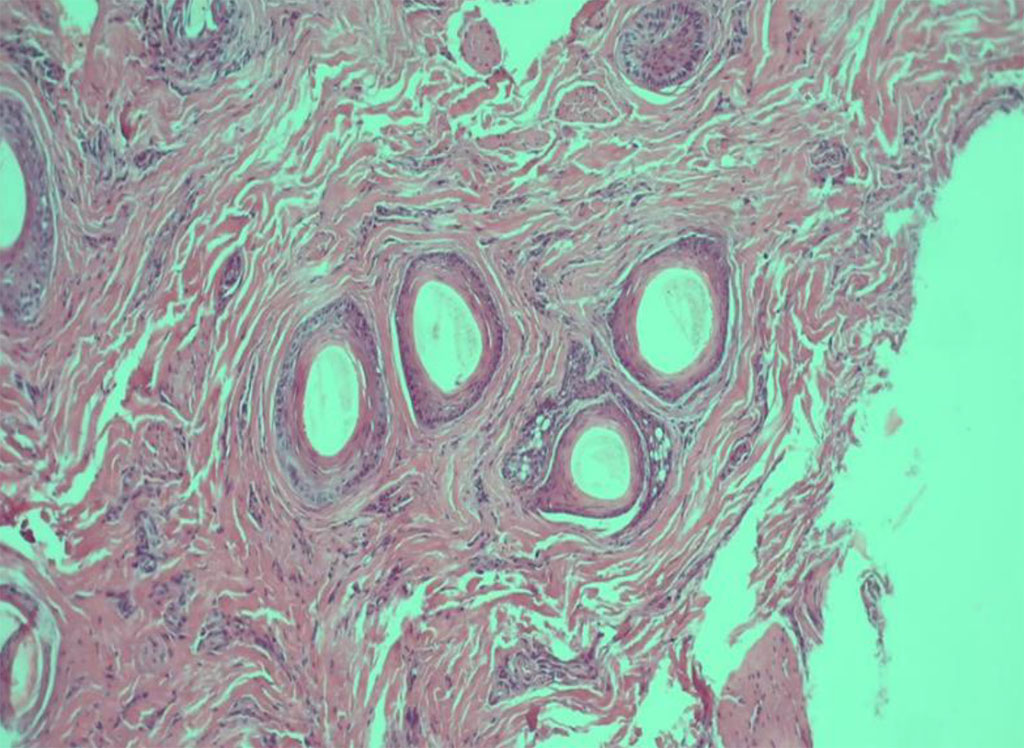
Fig.3 Histological picture of LPP (staining with hematoxylin and eosin)
Based on the totality of features, the histological picture corresponds to the follicular form of lichen planus. The treatment regimen was corrected; intralesional corticosteroid injections were prescribed once a month, oral cyclosporine at a dose of 3 mg/kg per day. During a treatment period of 3 months, positive dynamics were noticed: itching subsided, peripheral growth of lesions, the phenomena of perifollicular erythema and hyperkeratosis decreased significantly, and hair loss stopped. Treatment was continued with cyclosporine until the skin rashes were completely stabilized.
This clinical case demonstrates the need to conduct a histological examination in patients with scarring hair loss in order to select the most effective treatment method. The variety of forms of cicatricial alopecia and their common clinical manifestations create difficulties in differential terms and require an integrated approach to their diagnosis. Proper control of inflammation can prevent the progression of cicatricial alopecia.

|
||