Erfolgreich durch internationale Zusammenarbeit
PUBLIC HEALTH
DOI 10.35630/2023/13/2.404
Received 25 March 2023;
Accepted 19 April 2023;
Published 25 April 2023
Treatment
and Diagnostic Errors Made by Emergency Medical Services Personnel
During Hospitalization of Patients
Evgeniy
Barinov1,2  ,
Andrey Barinov1 ,
,
Andrey Barinov1 ,
Svetlana Voyevodina1 ,
Sergey Dzhuvalyakov2 ,
Inna Osipova 1,
Ruslan Kalinin1,2 ,
Olga Romanova 2,3 
1 A.I.Yevdokimov
Moscow State University of Medicine and Dentistry, Moscow;
2 RUDN University, Moscow;
3 A.P.Avtsyn Research Institute of Human Morphology, Moscow, Russia
 download article (pdf)
download article (pdf)
olgpharm@yandex.ru
ABSTRACT
The
aim of the study is to analyze treatment and diagnostic errors made
by emergency medical services personnel during hospitalization of
patients.
Materials
and Methods: The analysis was made based on 412 report sheets to run sheets, taken at one EMS substation for
one month. The sample included only report sheets for orders carried
out by EMS feldshers. Analyzed materials showed that 42 report sheets
contain defects in filling out the documentation: for example, 3 of
them did not indicate a referral diagnosis of the EMS team, and 39 –
final diagnosis of the hospital, and, therefore, they cannot be
included in the statistical data. Analysis of the remaining 370
report sheets showed that in 60 cases there was an overdiagnosis of
the disease, and in 31 cases the diagnosis was incorrect.
Conclusion: From the analyzed materials, it is possible to identify the main
treatment and diagnostic errors in the work of the EMS in cases of
patient hospitalization: Incorrect tactics of managing patients at
the prehospital stage due to overestimation/underestimation of
symptoms, non-core hospitalization or hospitalization in a non-core
hospital due to overestimation/underestimation of symptoms;
replacement of a nosological unit with its symptoms or complications.
Keywords: emergency medical services, defect in the provision of medical
services, prehospital stage
Background
Nowadays,
stories about harm to the health of patients gain the most popularity
in the media – doctors are accused of untimely or incorrect medical
manipulations or absence of such. This gives rise to numerous
lawsuits against medical professionals, private and public clinics,
making one think that medical services are not always provided by
qualified specialists.
However,
publication of the details of civil proceedings in the media,
constant increase in the number of lawyers of the corresponding
professional orientation and a number of other factors indicate the
fact that in most cases a high number of lawsuits against medical
organizations is not always an indicator of their poor performance.
Emergency
medical services (EMS) units, along with outpatient units, perform
the largest volume of medical services for the population, which is
related to the nature of its work and the tasks assigned thereto, the
primary of which is the provision of emergency medical services at
the prehospital stage.
Provision
of emergency medical services is characterized primarily by:
- lack
of time required for treatment and diagnostic manipulations;
- diagnostic
uncertainty under severe time constraints, which requires to start
the provision of services to a patient without a reliably verified
diagnosis;
- transience
of most emergency conditions and high risk of complications;
- change
of diagnosis in the first hours after the patient's admission to the
hospital after conducting examinations that are not available at the
prehospital stage;
Therewith,
in the work of EMS teams, unfortunately, there are various kinds of
errors and defects that lead to adverse consequences [1-4].
In
literature, there are various definitions of defects in the provision
of medical services. According to Tomilin V.V. and Sosedko Iu.I.,
defect in the provision of medical services means an improper
performance by a medical specialist of his/her professional duties,
which led to incorrect diagnosis, treatment of patient and led to an
adverse outcome [5]. Stetsenko S.G. provides the following definition
of defect – improper diagnosis, treatment, rehabilitation of
patient, organization of medical services, which led or could lead to
an adverse outcome of medical intervention. Semkin L.B., Filatov V.V.
and Gulyaev V.A. define defect in the provision of medical services
as poor-quality provision of medical services with errors in the
diagnosis and treatment of a patient or an omission in the
organization of medical services which had or could have a negative
impact on the treatment process and the patient's health [6].
In
our opinion, defect in the provision of medical services at the
prehospital stage means a violation of the treatment and diagnostic
process and the organizational and technical measures, expressed in
failure to comply with the established regulations, rules, customs
and traditions of business conduct adopted in medical practice,
non-compliance with medical procedures, clinical protocols and
recommendations, or the results of implementation thereof, whether or
not resulting in harm to the patient.
In
1999, I.V. Timofeev proposed a classification of defects at the
prehospital stage of the provision of medical services, which
includes not only a list of defects, but also reasons causing them.
1.
Classification of defects at
the prehospital stage
Defects
in the provision of medical services:
- failure
to perform emergency medical services (including resuscitation);
- delayed
performance of emergency medical services (including resuscitation);
- improper
performance of emergency medical services (including resuscitation);
- late
referral to inpatient treatment;
- improper
(unreasonable) transportation of patients;
- other
defects in the provision of medical services.
Defects
in evacuation:
- unreasonable
leaving of patients (wounded, injured) at the scene of the incident
when there are signs of a disease present;
- early
(not indicated) evacuation of patients (wounded, injured);
- late
evacuation (delivery) of patients (wounded, injured) to the stage of
the provision of qualified and specialized medical services;
- evacuation
for other purposes.
Defects
in diagnosis:
- underlying
disease (injury, damage) is not identified;
- combined
nature of a disease (competing diseases, comorbidities, background
injuries, damages) was not identified;
- leading
(in the case of lethal outcome – fatal) complication was not
identified;
- late
diagnosis of the underlying disease (wound, injury);
- late
diagnosis of the leading (in the case of lethal outcome – fatal)
complication;
- incorrect
diagnosis (underestimation of severity) of the condition of patients
(wounded, injured);
- other
defects in diagnostics.
Defects
in treatment:
- untimely
(not fully implemented) outpatient treatment;
- incorrect
prescription of drugs, other treatment methods;
- other
defects in treatment.
Other
defects at the prehospital stage:
- improper
maintenance of medical records;
- defects
in medical examination;
- other
defects.
2.
Causes of defects
- Inattentive
attitude towards patients;
- Violation
of deontological principles in relations with patients (and their
relatives);
- Insufficient
qualification of a medical specialist:
- low
level of clinical thinking of a doctor;
- inability
to logically comprehend the revealed data;
- inability
to formulate correct diagnosis based on clinical data;
- insufficient
level of professional (special) training, including little clinical
experience and lack of knowledge of the possible consequences of
specific methods of diagnostics and treatment;
- Late
seeking of medical attention;
- Shortcomings
in the organization of preventive, diagnostic and treatment
measures;
- Objective
difficulties in the performance of treatment and preventive
measures:
- Other
causes of defects in the provision of medical services.
Based
on literature, the most common defects occur during the provision of
emergency medical services (53.2%). Therewith, the number of defects
in the performance of professional duties by EMS doctors is quite
large. The most common diagnostic defects are expressed in incomplete
and insufficient examination of patients [7].
Such
a large number of defects arises due to the fact that the provision
of medical services at the prehospital stage causes certain
difficulties, primarily related to objective difficulties in
diagnosing patient's disease, establishing a diagnosis, and, as a
result, choosing the right treatment tactics. This is due to the
following factors:
- Limited
scope of diagnostic examinations. Usually, only such diagnostic
methods as glucometry, ECG and pulse oximetry are available to an
EMS specialist, which are sometimes carried out under difficult
conditions (interior of an EMS vehicle, public places, etc.), which
significantly complicates the diagnosis.
- Limited
call time. In Moscow, based on internal order, the time the team is
on call does not exceed 20 minutes, during which the team is
required to carry out not only diagnostic, but also treatment
measures. There is also a time standard for medical evacuation of
patients with acute infarctions and strokes to the hospital within
72 minutes from the moment the call was received at the station
(previously – from the moment the team arrived at the call site).
- Work
of EMS specialists alone due to a shortage of personnel. Despite the
fact that, in accordance with the Procedure for the Provision of
Emergency, Including Emergency Specialized, Medical Services,
approved by Order of the Ministry of Health of Russia dated June 20,
2013 No. 388н,
general feldsher and general physician teams should have at least
two medical specialists. However, usually, this requirement is not
met due to the high turnover and shortage of personnel, mobile teams
are not properly staffed, and EMS teams usually have only one
medical specialist. Such circumstances significantly complicate the
provision of medical services by EMS personnel, especially in
emergency situations.
- Frequent
conflicts with patients. In a number of cases, when an EMS team is
called, patients and their relatives, being in an extremely excited
emotional state, present certain requirements to the EMS personnel,
for example, unconditional hospitalization, including unreasonable
one. Often, in order to minimize conflict, medical specialists
comply with such requirements, including in coordination with higher
management. In such cases, in run sheets, a referral diagnosis is
made in a probabilistic form (“in question”), which often does
not correspond to the objective picture, is unmotivated and
unreasonable. Such referral diagnoses of EMS teams, being the cause
of conflicts with medical specialist of the emergency department of
hospitals, ultimately do not correspond to the final diagnosis
established in the hospital, thereby there is a discrepancy in
diagnoses, which indicates violations and errors in the diagnostics
of patient's disease at the prehospital stage.
Indicator
of discrepancy between EMS team and hospital diagnoses characterizes
the level of diagnostics and continuity in the work of EMS teams and
hospitals. The
indicator is calculated by the following formula (%):

The
recommended indicator is not more than 5%.
The
aim of the study is to analyze treatment and diagnostic errors made by
emergency medical services personnel during hospitalization of
patients.
Materials
and Methods
The
analysis was based on 412 report sheets to run sheets, taken at one
EMS substation for one month. The sample included only report sheets
for orders carried out by EMS feldshers.
It
was detected that 42 report sheets contain defects in filling out the
documentation. For example, 3 of them did not indicate a referral
diagnosis of the EMS team, and 39 – final diagnosis of the
hospital, and, therefore, they cannot be included in the statistical
data.
Analysis
of the remaining 370 report sheets showed that in 60 cases there was
an overdiagnosis of the disease and in 31 cases – diagnosis was not
correct.
Table
1. General results of in-house study
Concurrence
of diagnosis |
Incorrect
diagnosis |
Overdiagnosis |
Defects
in filling out report sheet |
Number
of cases |
%
of cases |
Number
of cases |
%
of cases |
Number
of cases |
%
of cases |
Number
of cases |
%
of cases |
| 279 |
68 |
31 |
7 |
60 |
15 |
42 |
10 |
| Total:
412 cases of patient hospitalization in Moscow hospitals |
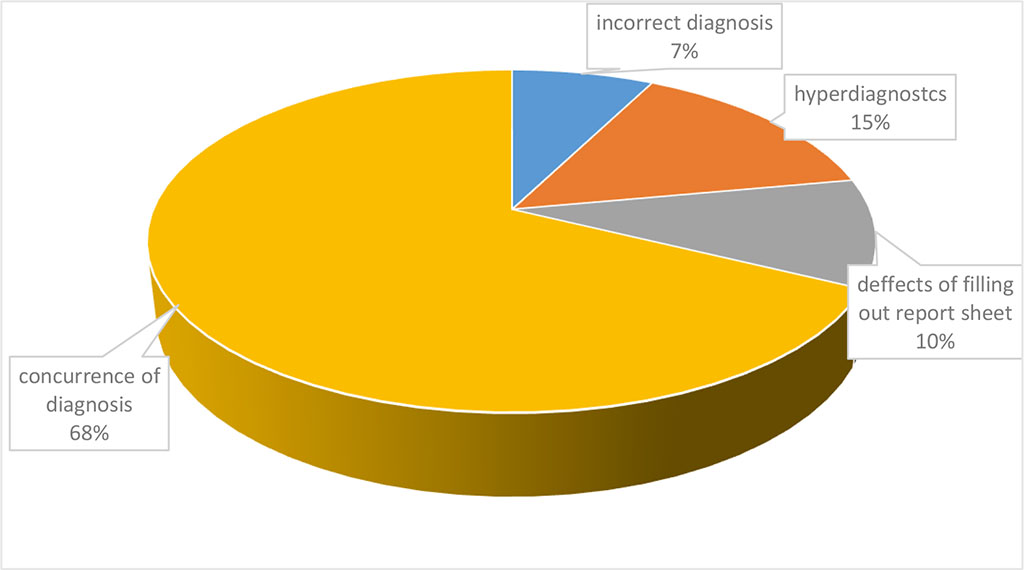
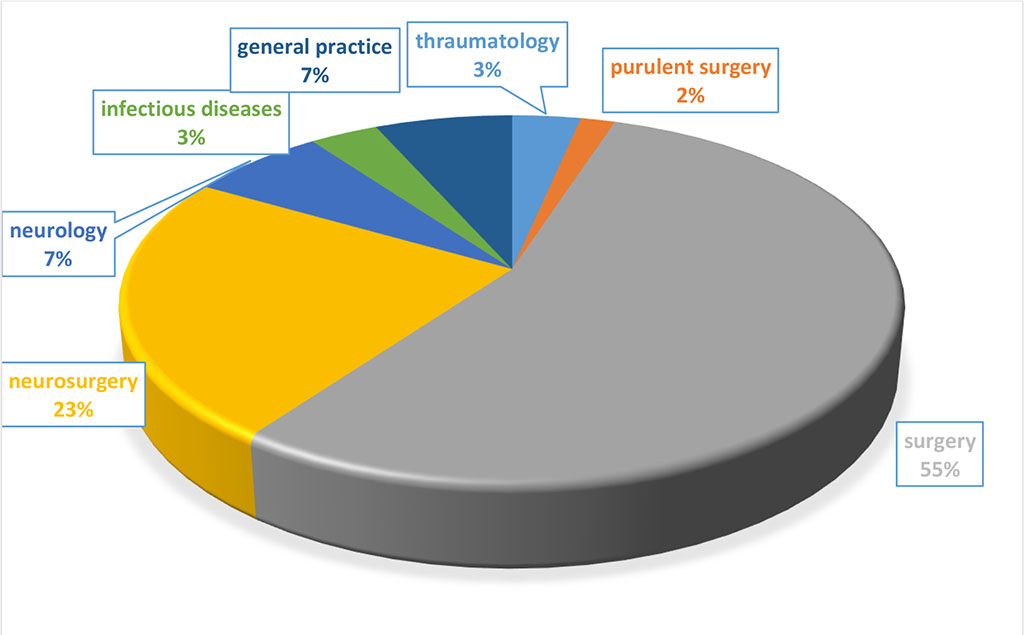
Diagram
1. General results of in-house study
If
we consider the frequency of incorrect clinical diagnosis of
individual nosological entity, then, as a result, we get the
following data presented in Table 2.
Table
2. Incorrect referral diagnosis of EMS teams for individual
nosologies
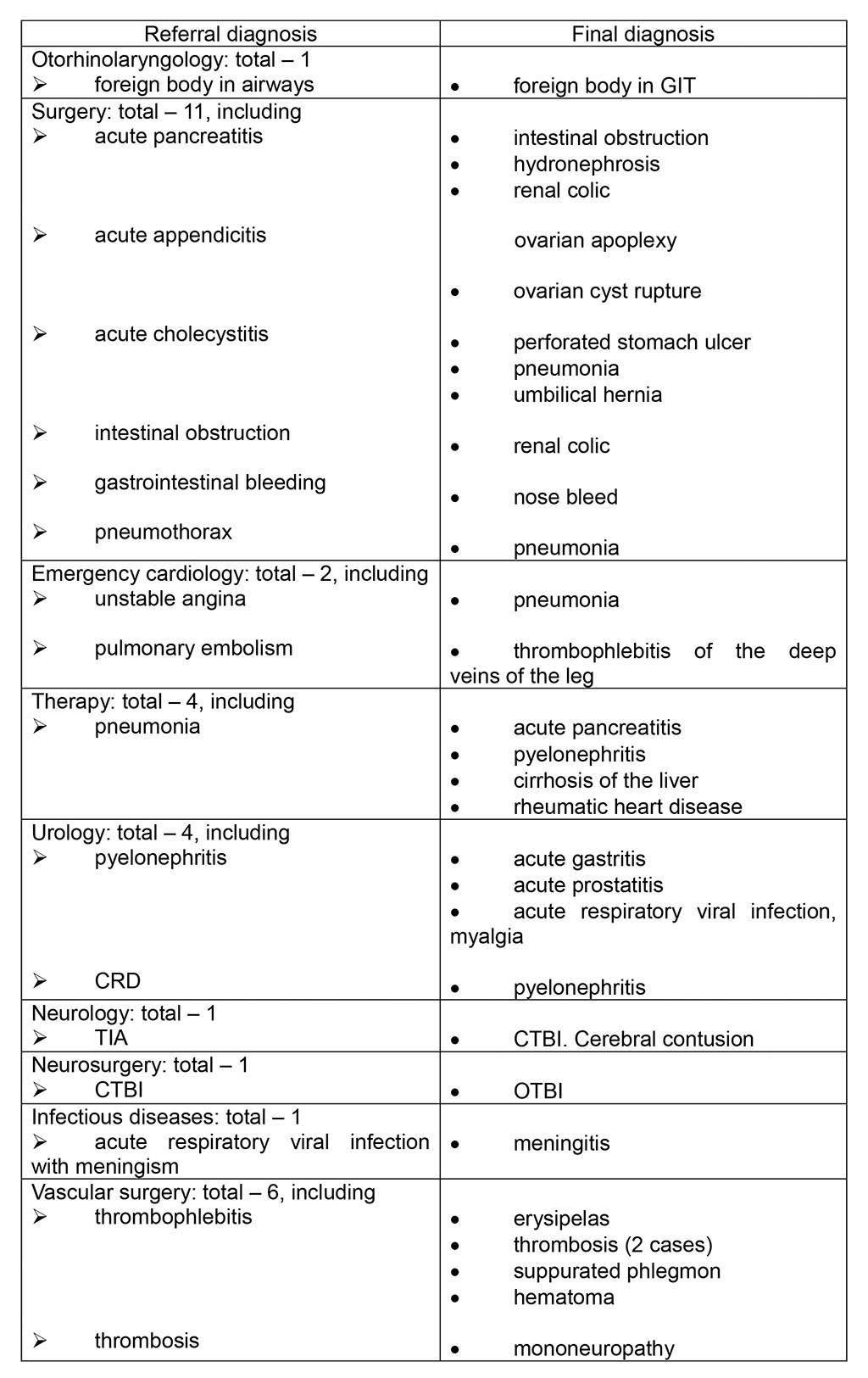
The
above data shows that the main treatment and diagnostic defects are:
- Incorrect
tactics of managing patients at the prehospital stage.
- Hospitalization
of patients in non-core hospitals.
- Lengthening
of the time required to make a correct clinical diagnosis and, as a
result, delay in the provision of medical services to patients in a
hospital. It is especially worth noting that doctors of admission
departments of hospitals are primarily obliged to exclude the
referral diagnosis of an EMS team.
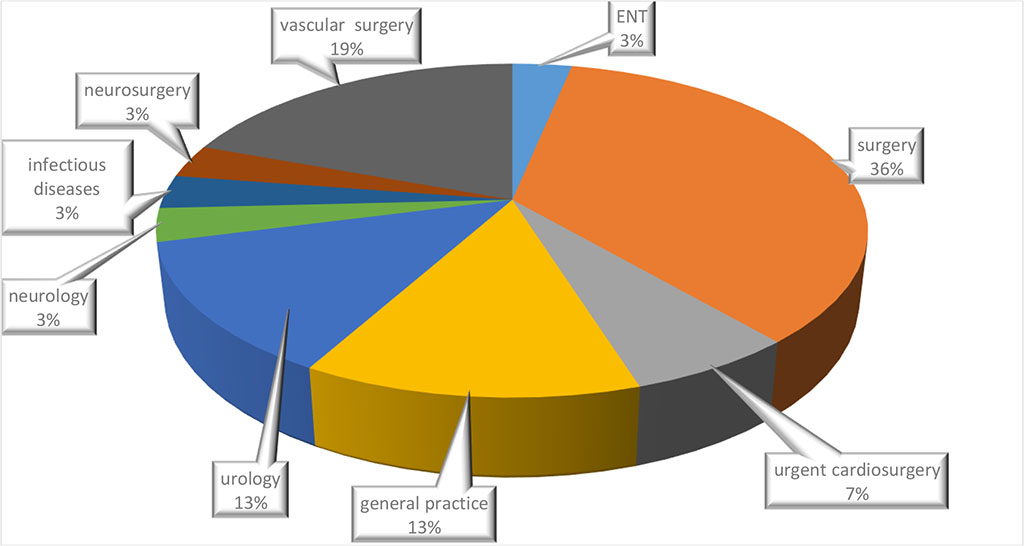
Diagram
2. Incorrect referral diagnosis of EMS teams for individual
nosologies
Table
3. Overdiagnosis by EMS feldshers of certain nosologies
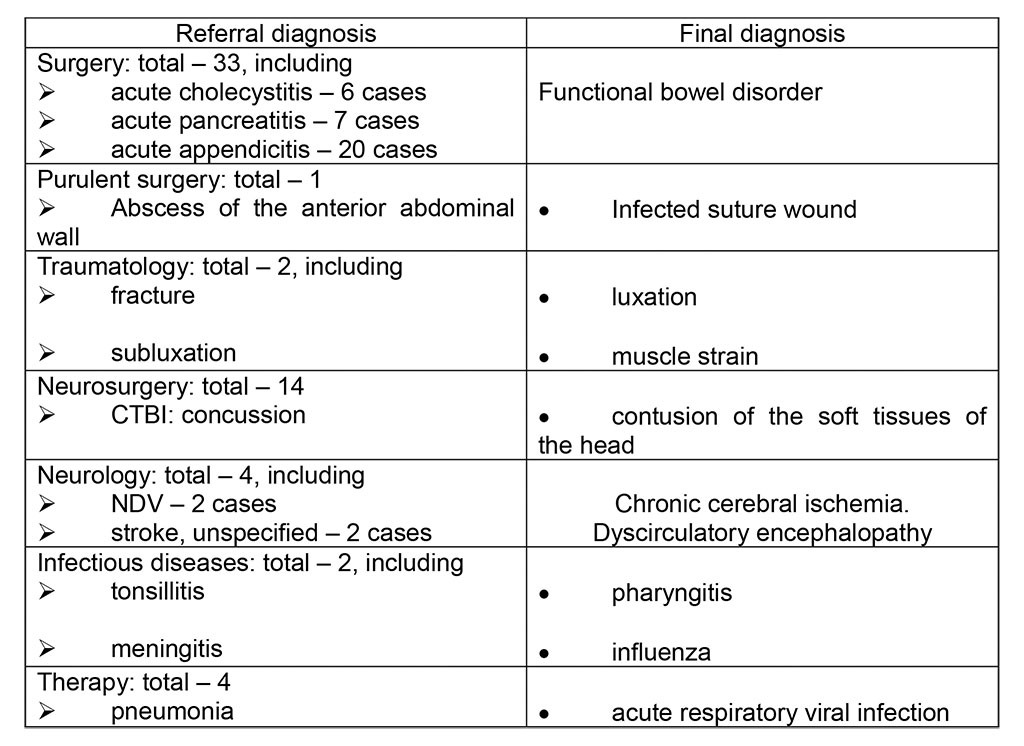
The
above data shows that the main treatment and diagnostic defects are:
- Incorrect
tactics of managing patients at the prehospital stage.
- Non-core
hospitalization of patients (patients did not require
hospitalization).
Diagram
3. Overdiagnosis by EMS feldshers of certain nosologies.
CONCLUSION
From
the analyzed materials, it is possible to identify the main treatment
and diagnostic errors in the work of the EMS in cases of patient
hospitalization.
- Incorrect
tactics of managing patients at the prehospital stage due to
overestimation/underestimation of symptoms;
- Non-core
hospitalization or hospitalization in a non-core hospital due to
overestimation/underestimation of symptoms;
- Replacement
of a nosological unit with its symptoms or complications.
REFERENCES
- Rodziewicz
TL, Houseman B, Hipskind JE. Medical Error Reduction and Prevention.
2022 Dec 4. In: StatPearls [Internet]. Treasure Island (FL):
StatPearls Publishing; 2022 Jan–. PMID:
29763131.
- Battard
J. Nonpunitive response to errors fosters a just culture. Nurs
Manage. 2017 Jan;48(1):53-55. - PMID: 28033214
DOI: 10.1097/01.NUMA.0000511184.95547.b3
- Robertson
JJ, Long B. Suffering in Silence: Medical Error and its Impact on
Health Care Providers. J Emerg Med. 2018 Apr;54(4):402-409.
PMID: 29366616 DOI: 10.1016/j.jemermed.2017.12.001
- Hines
S, Kynoch K, Khalil H. Effectiveness of interventions to prevent
medication errors: an umbrella systematic review protocol. JBI
Database System Rev Implement Rep. 2018 Feb;16(2):291-296.
PMID: 29419613 DOI: 10.11124/JBISRIR-2017-003481
- Tomilin
V.V., Sosedko Yu.I. Substantiation of the basic concepts of defects
in the provision of medical care. Sudebno-mrditsinskaya expertiza
(Forensic medical examination). 2000; 6: 4-8 [In Russ.]
- Guliaev
VA, Filatov VV, Semkin LB.Methodological basis for analysis of
shortcomings in rendering medical care. Voen
Med Zh. 2001;322(4):15-20. Russian. PMID: 11547659 [In Russ.]
- Tyagunov
D.V., Samoilichenko A.N. Characteristics of defects in the provision
of medical care based on materials of commission forensic medical
examinations Meditsinskoye pravo (Medical law). 2008;4: 26-29 [In
Russ.]
back
