- Home
- About the Journal
- Peer Review
- Editorial Board
- For Authors
- Reviewer Recognition
- Archive
- Contact
- Impressum
- EWG e.V.
Cite as: Archiv EuroMedica. 2026. 16; 1. DOI 10.35630/2026/16/Iss.1.011
Granulomatosis with polyangiitis is a rare systemic ANCA associated vasculitis that typically involves the upper respiratory tract, lungs, and kidneys. Gastrointestinal manifestations are uncommon and may lead to diagnostic confusion with inflammatory bowel diseases, particularly Crohn’s disease.
To present a diagnostically challenging clinical case of granulomatosis with polyangiitis with predominant gastrointestinal manifestations mimicking Crohn’s disease and to highlight the role of serological and histopathological assessment in establishing the correct diagnosis.
A detailed clinical evaluation was performed including laboratory testing, endoscopic examinations, cross sectional imaging, and histopathological analysis. Serological testing for ANCA was conducted, and the patient was assessed by a multidisciplinary team.
A 37 year old female presented with bloody diarrhea, hematemesis, abdominal pain, arthralgia, and oral ulcerations. Endoscopic and radiological findings suggested Crohn’s disease with segmental small bowel wall thickening and multiple gastric and colonic ulcers. Laboratory evaluation revealed anemia, leukocytosis, elevated inflammatory markers, and markedly elevated PR3 ANCA levels. Histopathological examination demonstrated chronic active inflammation consistent with vasculitis. The final diagnosis of granulomatosis with polyangiitis was established.
Granulomatosis with polyangiitis may present with predominant gastrointestinal involvement closely resembling inflammatory bowel disease. In patients with atypical gastrointestinal manifestations and systemic features, ANCA associated vasculitis should be considered, and extended serological and histopathological diagnostics are essential to avoid delayed or inappropriate treatment.
Keywords: Crohn’s disease, granulomatosis with polyangiitis, ANCA associated vasculitis, gastrointestinal involvement, case report
GPA, previously known as ‘Wegener's granulomatosis’, is an autoimmune disease that attacks both small and medium-sized blood vessels. Clinically, it is characterized by otolaryngological symptoms involving both the lungs and the kidneys. A key feature of GPA is the presence of ANCA in approximately 90% In approximately 90% of patients with generalized GPA, and approximately 60–70% of patients with localized GPA (e.g., limited to the upper respiratory tract). PR3-ANCA are highly specific for GPA and therefore, have high diagnostic value.
Conversely, Crohn's disease, is a chronic inflammatory condition that affects the GI tract resulting in changes from the mouth to the anus which may lead to extraintestinal complications. Typical symptoms include: diarrhea, abdominal pain, rectal bleeding, fever, weight loss, and fatigue. Initial laboratory assessments may identify inflammation, alongside screening tests for differential diagnoses. Measuring fecal calprotectin is valuable for excluding diseases in both adults and children. Endoscopy and cross-sectional imaging are used to confirm the diagnosis and determine the extent of the disease.
As both entities can manifest with generalised symptoms of weight loss and GI complaints, this may lead to misdiagnosis. This article illustrates the case of a patient with a clinical presentation resembling Crohn's disease, however the eventual diagnosis was GPA.
Despite the systemic nature of granulomatosis with polyangiitis, gastrointestinal involvement in this disease is rare and often underestimated. In cases where gastrointestinal symptoms predominate, the clinical presentation may fully mimic inflammatory bowel diseases, leading to diagnostic errors and delayed initiation of appropriate therapy. Diagnostic difficulties are particularly pronounced when endoscopic and radiological findings are consistent with Crohn’s disease and precede the development of typical pulmonary or renal manifestations of granululomatosis with polyangiitis.
The clinical relevance of this problem is determined by the fundamental differences in pathogenesis and therapeutic approaches between inflammatory bowel diseases and ANCA associated vasculitides. Delayed recognition of granulomatosis with polyangiitis in patients with predominant gastrointestinal symptoms may result in progression of systemic organ involvement and inappropriate treatment.
The aim of this clinical observation is to demonstrate a diagnostically challenging case of granulomatosis with polyangiitis presenting predominantly with gastrointestinal symptoms and an endoscopic picture resembling Crohn’s disease, and to emphasize the importance of serological and histopathological methods in establishing the correct diagnosis.
The novelty of this work lies in the detailed description of a clinical case of granulomatosis with polyangiitis with predominant gastrointestinal manifestations that at the stage of initial diagnosis completely mimicked Crohn’s disease based on clinical presentation, endoscopic findings, and imaging. The article consistently demonstrates that the combination of segmental small bowel involvement, multiple ulcerations of the gastric and colonic mucosa, anemia, and inflammatory changes may mask an underlying systemic vasculitis. Of particular value is the documented identification of an extremely high PR3 ANCA titer and subsequent histopathological confirmation of a vasculitic process, which allowed reconsideration of the initial diagnostic concept and modification of the therapeutic strategy.
The relevance of this work is determined by the high risk of diagnostic errors in atypical presentations of systemic vasculitides with gastrointestinal involvement. Crohn’s disease and granulomatosis with polyangiitis may have overlapping clinical and endoscopic features, yet require fundamentally different treatment approaches. The presented case demonstrates clinical and laboratory features in which standard gastroenterological diagnostic reasoning proves insufficient and highlights the need for early inclusion of serological and morphological methods in the diagnostic algorithm. The work has practical significance for gastroenterologists, rheumatologists, and clinicians involved in the multidisciplinary diagnosis of complex inflammatory diseases.
A 37-year-old female patient was admitted to the hospital with diarrhea in the presence of blood, nausea, hematemesis, abdominal pain, and joint pain.
The patient was previously admitted to an Endocrinology Clinic and diagnosed with a left adrenal gland lesion. A few days after being discharged from the hospital, she experienced bilateral lower limb muscular pain in the calves and thighs. This was followed by migrating ankle and knee joint pain, which progressed to the small joints of both hands, as well as the large joints of the upper and lower limbs.
Due to the suspicion of rheumatoid arthritis, (in the absence of immunological diagnostic conformation), the patient administered NSAIDs and methotrexate at a dose of 10 mg for 3/52. The medication was discontinued 7-10 days prior to being admitted to hospital by a Rheumatologist. In addition, the patient was prescribed amoxicillin and clavulanic acid (3x1g) for bilateral ear inflammation, resulting in oral ulcers making it impossible to eat and drink.
In association with the above clinical symptoms, alternative differential diagnoses were considered including; chronic connective tissue disease – SLE, rheumatoid arthritis, vasculitis and overlapping syndromes. Predominant GI symptoms and changes on CT scanning suggesting small bowel inflammation, i.e., segmentally thickened wall of the small intestine up to 6 mm (two loops) in the right iliac and lower abdomen, with slight blurring of the surrounding fat tissue - Crohn's disease and ulcerative colitis.
During hospitalization, a worsening anemia and symptoms of bleeding from the upper and lower gastrointestinal tract were observed, therefore the patient was transfused with 2 units of group-compatible red blood cells without complications. This results in an increase in hemoglobin concentration to 10 g/dl.
During the diagnostics, endoscopic examinations were performed showing numerous flat ulcers in the sigmoid colon with a base covered in fibrin measuring 5-10 mm, and the mucosa between the ulcers appeared normal and shiny, with preserved vascular pattern. (Figure 1 and 2)
Figure. 1 and 2. Investigative Gastroscopy showing 1-2 mm rectal ulcers with the bases covered in fibrin.
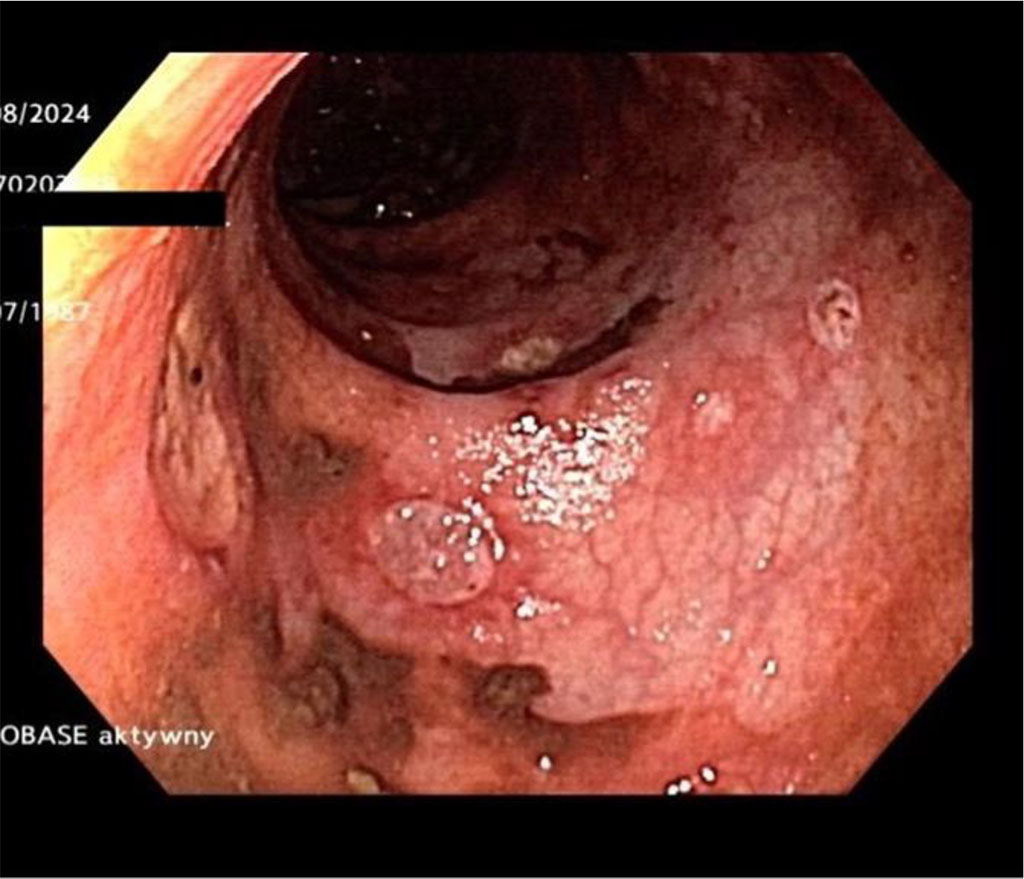
Figure 1
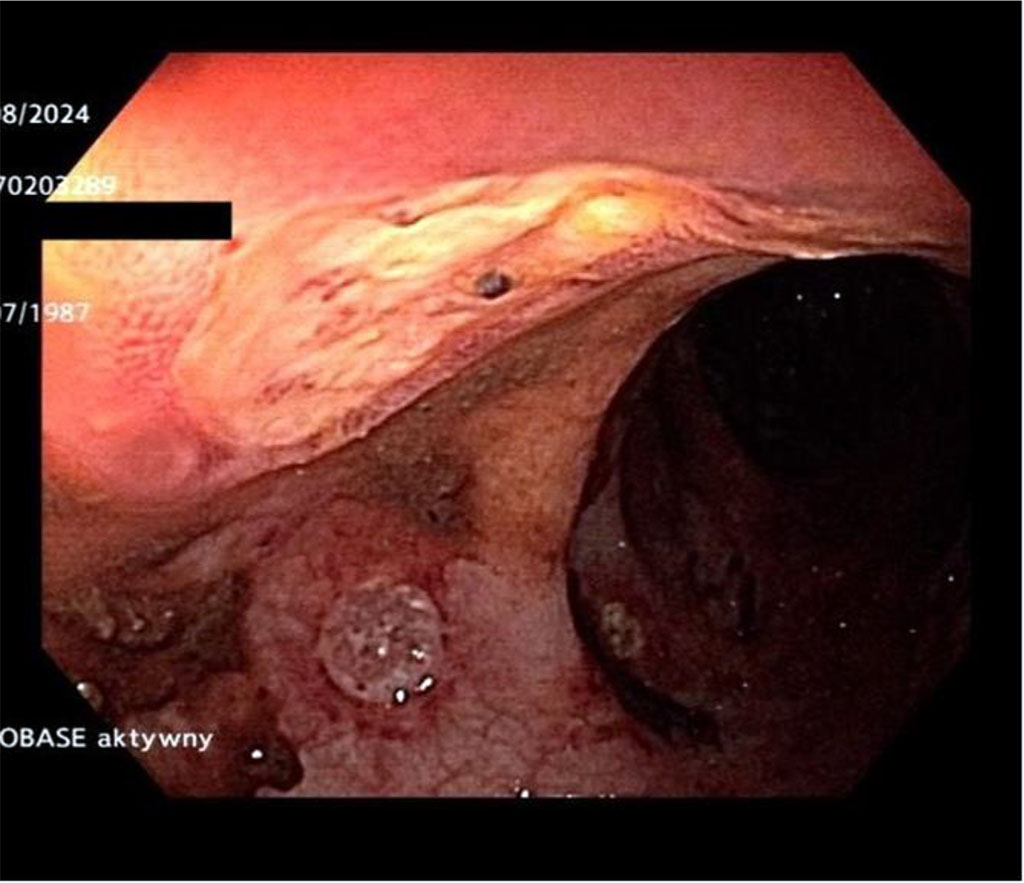
Figure 2
The mucous membrane of the antrum, body, fundus, and subcardial area were inflamed and erythematous (Figure 3). The oral cavity displayed a round, regular ulceration on the palate with a fibrinous base.
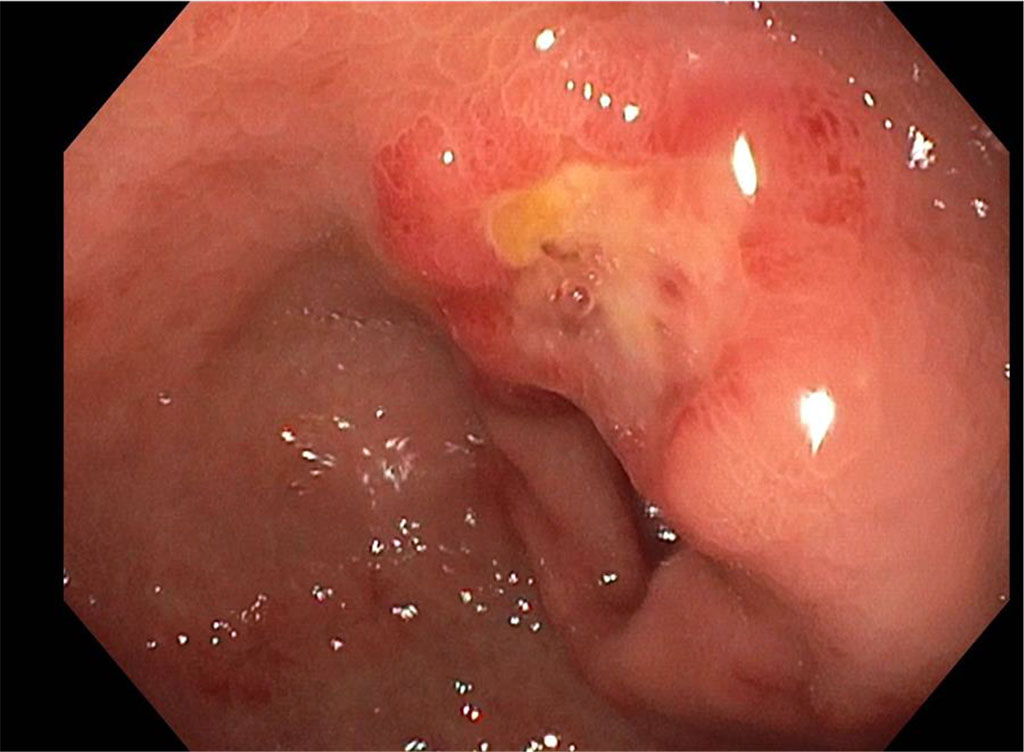
Figure 3. Further Gastroscopy findings showed deviations in the Antrum around the lesser curvature of the Pylorus, including a flat ulcer with a fibrinous base.
The patient was assessed by an Otolaryngologist and two ulcerations were found on the palate and tongue during the examination. An otoscopic examination showed signs of left ear congestion alongside slightly asymmetrical hearing (Figure 4)

Figure 4. Signs of left ear congestion alongside slightly asymmetrical hearing
The MR enterography with segmental enhancement (up to about 2 cm long), of the mucosa in 3-4 locations in the ileum. The changes widespread and accompanied by subtle edema of the submucosal layer. In addition, some hyperemia of the mesentery was observed with no fistulas or abscesses present. (Figure 5)
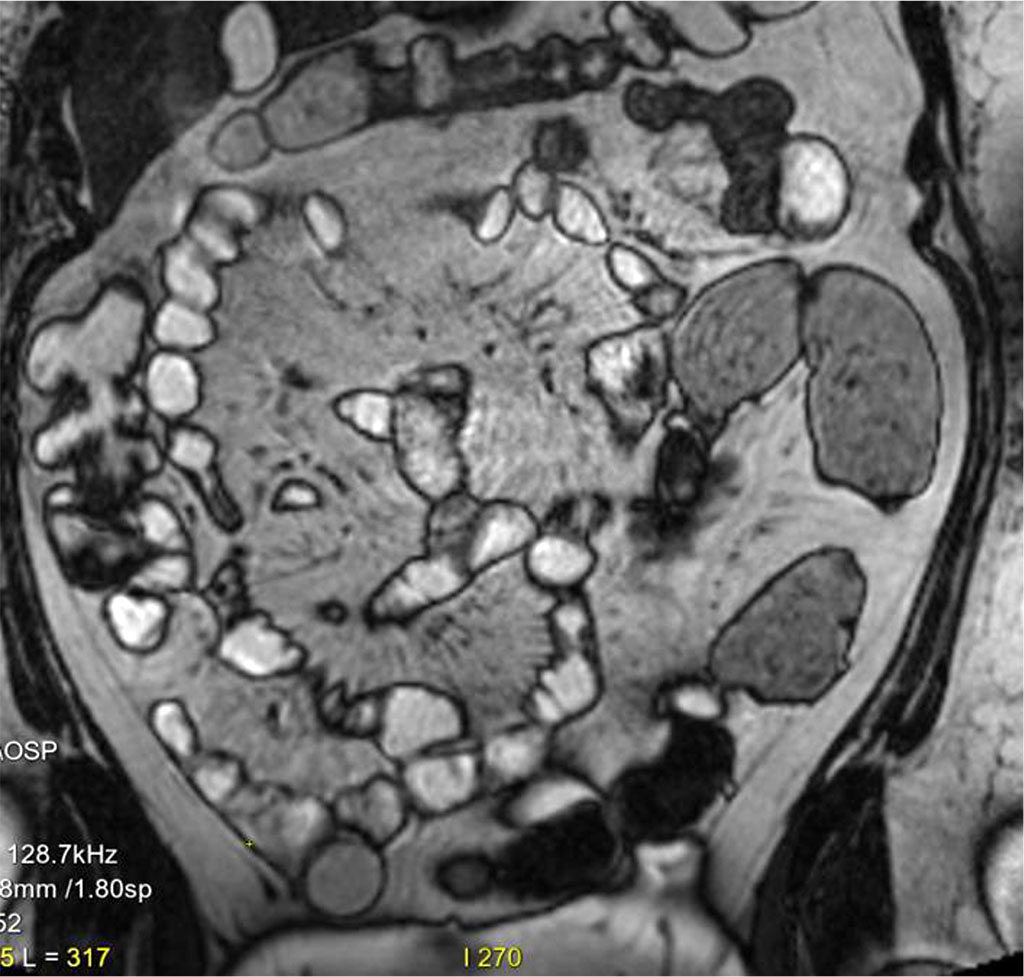
Figure 5. Segmental enhancement (up to about 2 cm long), of the mucosa in 3-4 locations in the ileum. The changes widespread and accompanied by subtle edema of the submucosal layer.
Proximal to the strictures, an osseous change measuring 38 x 12mm with a high signal in T2-weighted sequences and slightly elevated in T1-weighted sequences was observed on the anterior wall of the sigmoid colon, which showed slightly heterogeneous contrast enhancement. Therefore, a suspicion of an endometriosis focus was raised (Figure 6). During the gynecological consultation, no significant deviations were noted.
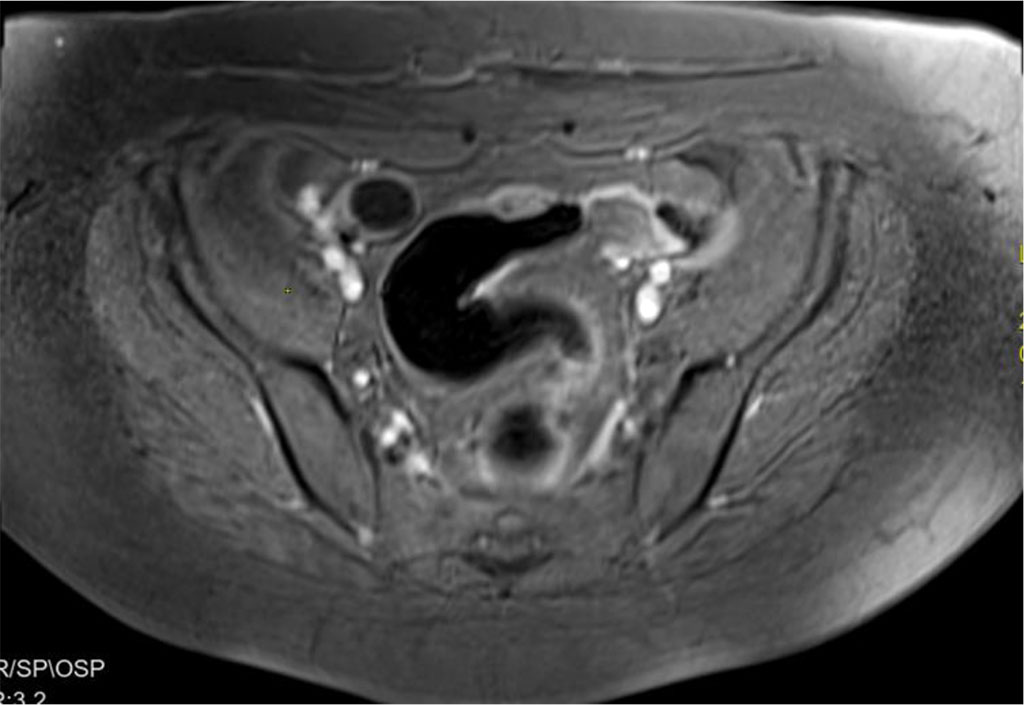
Figure 6. Suspicion of an endometriosis focus
The remaining deviations in laboratory tests are included in Table 1.
Table 1. Remaining deviations in laboratory tests
| Test: | Results |
| PR3-ANCA | 1862,7 CU |
| ASCA IgA | 1:000 |
| WBC | 13,02 |
| Hgb | 9,6 g/dl |
| MCV | 79,5 |
| D-dimer test | >10000 ng/mL |
| Urine sample | Proteinuria, Erythrocyturia |
| The urine 24-hour volume test | Protein 2.72 g/day |
| CT PA | No evidence of PE |
Treatment with sulfasalazine 4 g orally per day and hydrocortisone 4x100 mg IV was initiated with moderate improvement.
Microscopic examination results revealed chronic active inflammatory infiltrates with the presence of granulocytes, as well as features of atrophy and metaplasia. There were no signs of dysplasia, granulomas, or mycobacteria in the Ziehl-Nielsen staining.
A diagnostic kidney biopsy was planned; however, this was postponed due to elevated blood pressure measurements and persistent diarrhea. Anti-hypertensive treatment was optimized with positive effect. IV Hydrocortisone was administered which was converted to oral prednisolone (80 mg/day) on day 10 of treatment. Loperamide was added, resulting in more frequent bowel movements (Currently 2-3 bowels movement per day).
The overall picture supported the diagnosis of granulomatosis with vasculitis hence, the patient was referred for further treatment to the Rheumatology Clinic the Ministry of the Interior and Administration, where the diagnosis was confirmed. The patient received rituximab, resulting in sustained clinical improvement . At one-year follow-up, remains in remission.
In a retrospective pathological analysis, a discrete change was noted superficially in the submucosa that could be a granuloma with centralized fibrinoid necrosis. (Figure 7)
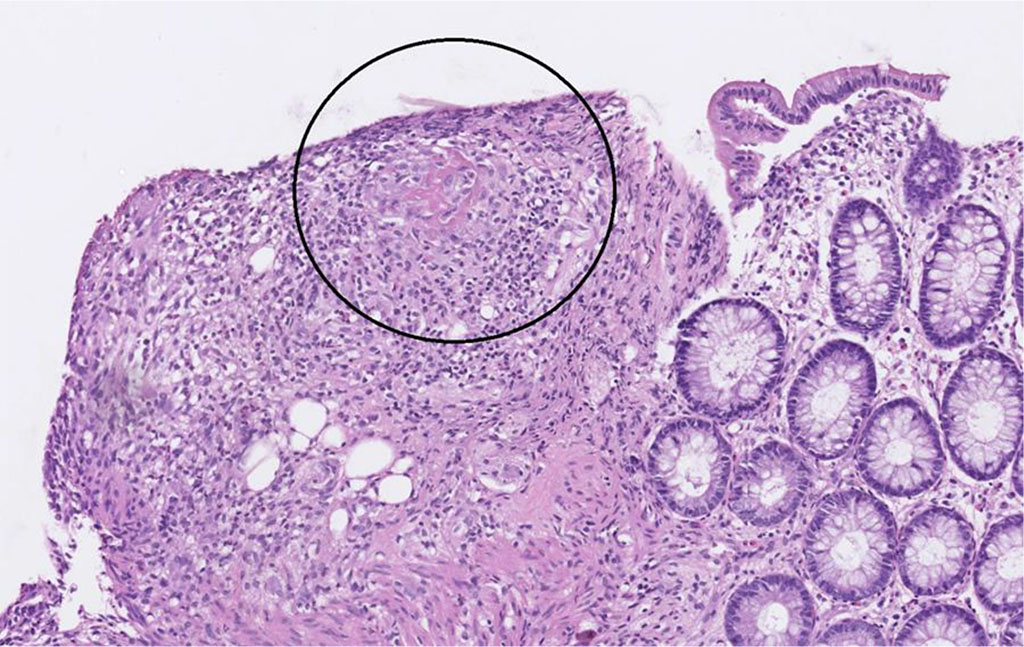
Figure 7 Discrete change in the submucosa that could be a granuloma with centralized fibrinoid necrosis.
Gastrointestinal involvement in granulomatosis with polyangiitis is described as a rare manifestation of the disease and may obscure its systemic nature [1,2]. In the present clinical case, gastrointestinal symptoms dominated the clinical presentation and were associated with endoscopic and radiological findings typical of Crohn’s disease, which significantly complicated early diagnosis. Segmental small bowel wall thickening and multiple ulcerations of the gastric and colonic mucosa were consistent with an inflammatory bowel disease pattern, in line with previously reported cases of diagnostic confusion between GPA and Crohn’s disease [1].
At the same time, the patient exhibited systemic manifestations not characteristic of isolated inflammatory bowel disease, including migratory arthralgia, otolaryngological involvement, anemia, and signs of renal impairment. The detection of a markedly elevated PR3 ANCA level had key diagnostic significance, as these antibodies have high specificity for granulomatosis with polyangiitis [2]. These findings necessitated revision of the initial diagnostic concept.
Histopathological examination demonstrated features of chronic active inflammation consistent with a vasculitic process, and retrospective reassessment revealed changes compatible with granulomatous inflammation and fibrinoid necrosis. Similar morphological findings have been reported in cases of gastrointestinal involvement in GPA and may be absent in initial biopsy specimens [1].
This clinical observation confirms that isolated interpretation of endoscopic and imaging findings may be insufficient in patients with suspected inflammatory bowel disease, particularly in the presence of systemic symptoms. The combination of gastrointestinal manifestations with positive ANCA serology should prompt consideration of ANCA associated vasculitis and expansion of the diagnostic algorithm [2,3].
This case demonstrates that granulomatosis with polyangiitis may present with predominant gastrointestinal manifestations that closely mimic Crohn’s disease not only clinically, but also endoscopically and radiologically. The presented observation highlights that the coexistence of segmental intestinal lesions, mucosal ulcerations, anemia, and systemic inflammatory features should prompt consideration of ANCA associated vasculitis, even in the absence of classic pulmonary manifestations. The identification of markedly elevated PR3 ANCA levels, renal involvement, and vasculitic changes on histopathological reassessment proved decisive for establishing the correct diagnosis and initiating appropriate immunosuppressive therapy. This case underscores the clinical importance of early multidisciplinary evaluation and expanded serological and histopathological diagnostics to avoid delayed or inappropriate treatment in patients with atypical inflammatory bowel disease like presentations.
The patient provided written consent for the anonymous publication of the case study.
Conceptualization and methodology: Adam Przybyłkowski, Robert Kucharski
Literature review and data extraction: Adam Przybyłkowski, Robert Kucharski, Katarzyna Celińska-Dzikowska
Writing – original draft preparation: Robert Kucharski, Katarzyna Celińska-Dzikowska, Bartosz Kucharski
Writing – review and editing: Adam Przybyłkowski, Robert Kucharski
All authors read and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Artificial Intelligence had been used for the purpose of style and language correction.
The authors declare no conflict of interest.
No funding was received to conduct this study.

|
||