- Home
- About the Journal
- Peer Review
- Editorial Board
- For Authors
- Reviewer Recognition
- Archive
- Contact
- Impressum
- EWG e.V.
Cite as: Archiv EuroMedica. 2025. 15; 1. DOI 10.35630/2025/15/1.113
Relevance: There are no reports in the literature on the relationship between the dimension of the mandibular angle and the freeway space. Knowledge of such a relationship would facilitate the design process of relaxation splints, which should fit within its limits.
The aim of the study: to examine the relationship between the size of the freeway space measured on premolars at different values of angle of the mandible.
Methods: Cephalometric images were utilized to explore the relationship between the angle of mandible and the freeway space. The angle of mandible was measured on the images. Freeway space was determined using an electronic caliper and occlusal separators in the posterior segment. The results underwent statistical analysis using the Statistica software.
Conclusions: 1.This analysis demonstrated a correlation between the mandibular
angle and the size of the freeway space in the lateral segment.
2.
Knowledge of the size of the freeway facilitates measurement of the
height of the relaxation splint.
Keywords: Mandibular angle, resting crevice, correlation analysis, relaxation splint, bruxism.
The anatomy of the mandible undergoes significant changes during human development. These changes also affect the angle of the mandible. At birth, this angle is 150°- 160°. With age, its value decreases, the ramus of mandible in relation to body of mandible takes on a more vertical position reaching an angle of 120°-130° in adulthood. The development of the craniofacial region has its fundamental beginning between 21 and 25 day of fetal life [1,2]. At this time, five facial processes arise from the mesenchyme from the fourth embryonic leaf and these are the even maxillary processes, the even mandibular processes and the frontonasal process (also known as the frontonasal prominence). These surround the stomodeum and then the primary oral cavity at a later stage [3]. In the fourth week of embryonic life, after the mandibular processes have fused, the mandible and lower lip are formed. The chin prominence, coronoid process and condylar process are formed between 10 and 11 weeks of fetal life. Synchondrosis between right and left part of mandible is possible due to an increase in the mandibular dimension in width. Ossification of synchondrosis occurs at 1 year of age. The ramus of mandible of the newborn is short and wide. The mandible has a large angle and a smaller condylar process and a larger coronoid process [2,4]. The main growth processes of the mandible take place in the cartilage of the condylar process and through the apposition on the posterior surface of the ramus of the mandible [3]. In the 5th week of embryonic life, the beginning of the development of the temporomandibular joint occurs. At week 7, the articular surface and articular disc develop. Between weeks 9 and 11 the articular capsule is formed, then week 10-11 is the period of development of the condylar process and week 10-12 the upper and lower compartment of the temporomandibular joint are formed. The relationship of the maxilla and mandible changes during individual development [2,4]. Up to the sixth week of gestation, the mandible occurs in a retro position in relation to the maxilla (embryonic retrogenia). Intensive growth of the mandible occurs with the formation of the secondary palate, leading to the development of embryonic progenia, the anterior position of the mandible in relation to the maxilla. In the following developmental periods, the maxilla grows much faster than the mandible, with the result that the child is born with a physiological retrognathia, which, under normal conditions within the first four months of life, is realigned [6,7]. The primary displacement of the mandible (downwards and forwards) occurs as a result of its actual growth. The growth of the structures of the middle cranial fossa, referred to as secondary displacement, results in its anterior repositioning [5,6]. The anterior displacement of the maxilla following the growth of the middle cranial fossa structures is significantly greater, resulting in a posterior relationship of the mandible to the maxilla under normal occlusal conditions [5,6].
The individual development of the mandible during childhood and adolescence is caused initially by the development of the deciduous dentition, the implementation of hard foods, later by the replacement of the dentition with permanent teeth and hormonal changes during puberty.
In adulthood, the mandible reaches its final form, which then changes due to ageing and the appearance of retrograde changes [1,2,4,5]. One important factor in the change in the size of the gonial angle during biomorphosis is bone atrophy, which results from the predominance of resorption processes due to the loss of functional stimuli from lost teeth. We distinguish between complete atrophy, i.e. uniform atrophy of the entire alveolar process, and partial atrophy, uneven atrophy of the alveolar process.
With regard to the cause, we can divide into senile atrophy, atrophy from hypofunction and atrophy from hyperfunction. The magnitude of the atrophy depends on, among other things, the age of the patient, tooth loss, hygiene and diet, general health and immunity. In the mandible, bone atrophy progresses in the anterior teeth from the vestibular side and in the lateral teeth from the oral cavity proper, resulting in an apparent elongation of the mandible. The angle of the mandible also changes, which enlarges due to, among other things, the pull of the masseter and medial pterygoid muscles [9].
The structure of the craniofacial region and its remodelling during biomorphosis often influences the treatment method used. Often, the clinician is faced with choosing the type of treatment depending on its structure. One of the practical problems is the treatment of bruxism. Bruxism has been a controversial phenomenon for years. The controversy concerns both the causes, treatment options and the qualification of this condition. Recently, a debate has arisen as to whether bruxism is a condition or a symptom. There is consensus on its multifactorial nature of the condition. In the past, morphological factors such as occlusion and the anatomy of the osteoarticular structures were considered the main causative factors of bruxism. Today, these factors play a minor role. According to current theories, the aetiopathogenesis of bruxism is primarily related to impaired masseter muscle tone. To date, bruxism has been, and often is, viewed as a occlusal parafunction. Currently, the various scientific consensus boils down to one thing - bruxism, in its essence, has a cerebral rather than a occlusal cause [6]. The use of a relaxation splint, the thickness of which should not exceed the dimension of the freeway space, is indispensable [6]. In the literature, we do not find reports on the relationship between the dimension of the angle of the mandible and the freeway space. Knowledge of such a relationship would facilitate the process of designing relaxation splints, which should fit within its limits.
The aim of this study was to determine whether the measure of angle of mandible influences the dimension of the freeway space.
21 patients including 13 females and 8 males were included in the study. Angle of manmdible and freeway space were measured three times.
Fig.1 Thermoformable flexible plate, 3mm thick.

Fig.2 The cut-out occlusal separator.
Freeway size was measured in a sitting position in the dental chair with the head resting against the headrest. The dental arches were unclenched by two occlusal separators (Fig. 2) cut from a flexible thermoformable plate (Fig. 1), 3mm thick, placed between the upper and lower first molars on either side of the dental arch (d.16, d.46 and d.26, d.36) (Fig. 4.1). The freeway space was measured between the mesial edge of the buccal cusp of the upper first premolar and the distal edge of the buccal cusp of the lower first premolar (Fig. 5) using an electronic calliper (Fig.3) to the accuracy of 0.01 mm.

Fig.3 Measurement of thermoformable plate thickness by electronic calliper (Preciva).
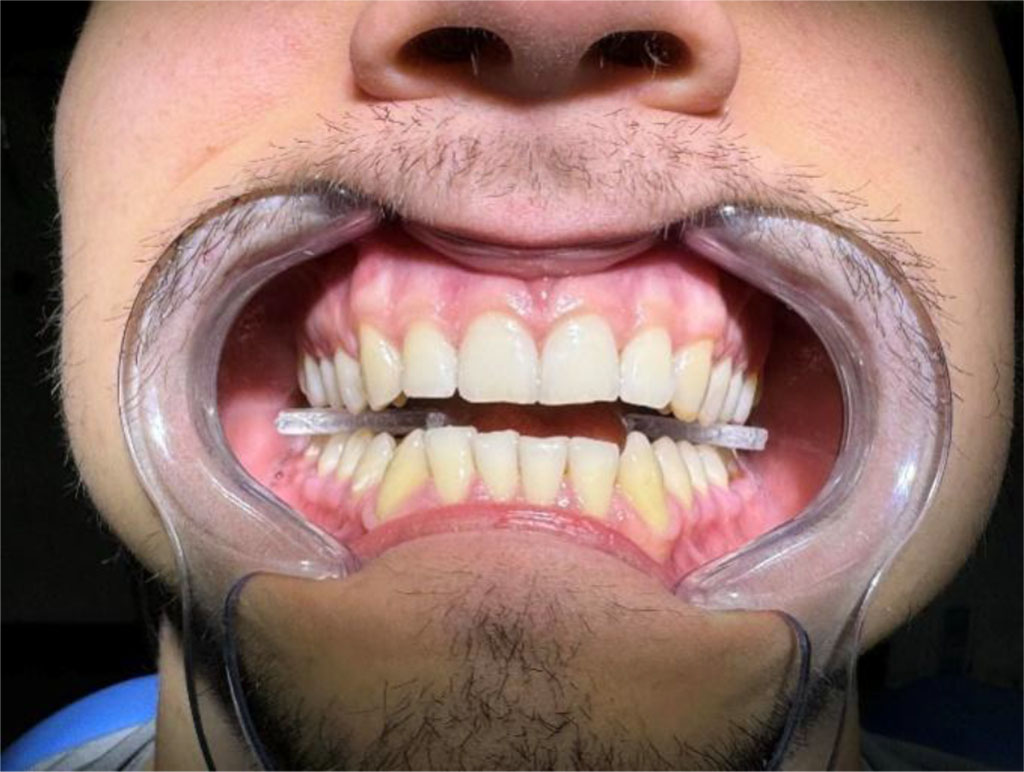
Fig.4.1 Patient with occlusal separators in occlusion.

Fig.4.2 Measurement of a freeway space.

Fig.5 Freeway space measurement points.
The analysis of the angle of mandible was based on cephalometric radiographs (Fig. 6). Radiographs were taken with the Gendex GXDP-700 in the maximal intercuspidation. The reference lines MT1 and MT2 were determined on them using Schwartz cephalometric analysis. MT1 corresponds to the tangent to the inferior margin of the body of mandiblepassing through the gnathion point and the top of the tuberosity of the attachment of the masseter muscle. MT2 is the tangent to the posterior edge of the ramus of mandible, defined by the posterior edge of the angle of mandible and the posterior edge of the mandibular head.

Fig. 6 Cephalometric image with MT1 and MT2 lines marked.
| Patient | Angle of mandible | Freeway space (mm) |
| 1 | 109 | 3,11 |
| 2 | 110 | 3,22 |
| 3 | 114 | 3,19 |
| 4 | 115 | 3,27 |
| 5 | 116 | 3,12 |
| 6 | 117 | 3,15 |
| 7 | 118 | 3,15 |
| 8 | 120 | 3,28 |
| 9 | 120 | 3,50 |
| 10 | 121 | 3,68 |
| 11 | 122 | 4,24 |
| 12 | 124 | 4,39 |
| 13 | 124 | 4,12 |
| 14 | 125 | 4,36 |
| 15 | 126 | 4,54 |
| 16 | 127 | 4,48 |
| 17 | 128 | 4,52 |
| 18 | 130 | 4,69 |
| 19 | 133 | 5,51 |
| 20 | 135 | 6,33 |
| 21 | 135 | 5,48 |
Fig.7 Comparison of angle of mandible and freeway space measurements in 21 patients
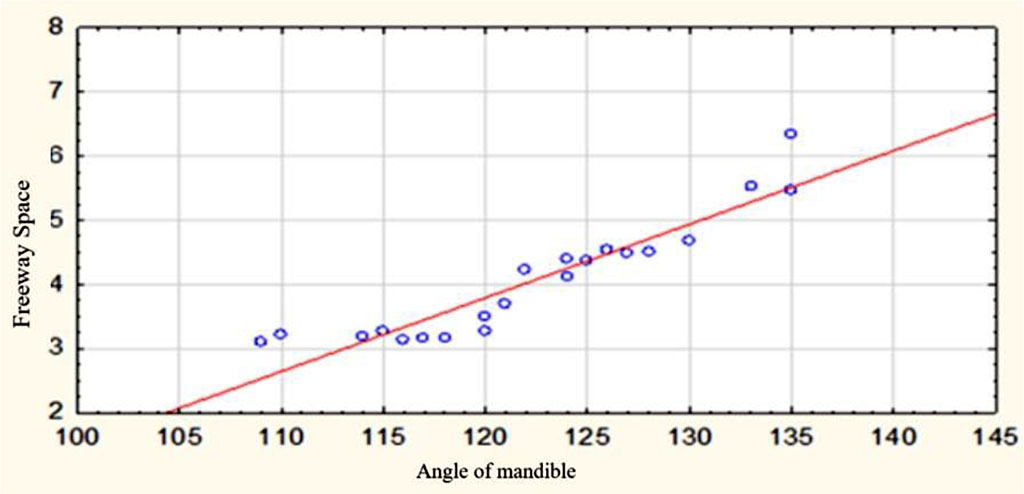
Fig.8 Freeway space in relation to angle of mandible
For the study group, the mean value of angle of mandible was 122.33°. Mean value of freeway space - 4.06 mm. Spearman's rank correlation coefficient - 0.65. For an angle of mandible approaching 110-120, the value of freeway space averaged 3.22(1)mm. For angle of mandible 121-135, the value averaged 4.695 mm.

|
||