- Home
- About the Journal
- Peer Review
- Editorial Board
- For Authors
- Reviewer Recognition
- Archive
- Contact
- Impressum
- EWG e.V.
We examined 40 patients with neuropathic (group 1, n=20) and neuroischemic (group 2, n=20) diabetic foot. Before surgical treatment, we studied the content of cytokines (TNF-α, IFN-γ, IL-1β, IL-6 and IL-10) and eicosanoids (LTB4 and PGE2) in the exudate of the ulcer discharge. Pathogenetic mechanisms of inflammation disorders in patients with neuropathic and neuroischemic forms of diabetic foot are different. The neuropathic form is characterized by an increase in the level of TNF-α and IL-6 in the wound exudate, inhibition of the IL-1β and IL-10 secretion, and the predominance of LTB4 in contrast to inhibition of PGE2 synthesis. At the same time, the formation of CD8+ is inhibited as well as the switching of the neutrophilic phase to the macrophage phase by maintaining the conditions for the differentiation of M1 macrophages. In the neuroischemic form, we revealed hyperproduction of IL-1β, IL-10, IFN-γ, CD4+ with inhibition of IL-6 secretion and eicosanoids imbalance (PGE2 prevail over LTB4). This disrupts the differentiation of M2 macrophages. All identified disorders may be due to the persistence of various neutrophil phenotypes in the wound.
Keywords: diabetic ulcer, inflammation, neutrophils, macrophages, cytokines, eicosanoids
Diabetic foot ulcer (DFU) is a serious complication of diabetes mellitus (DM). According to experts, they occur in 15% of patients with diabetes, precede 84% of all lower leg amputations in this category of patients, and are related with a high (42%) 5-year mortality of patients [1 -5].
Numerous studies on the pathophysiology of DFU and, in particular, the role of inflammatory cell populations in the wound, revealed a number of disorders in the regulation of nonspecific protective functions of leukocytes: defects in recruitment and chemotaxis, decreased activity of phagocytosis and killing of bacteria, impaired neutrophils apoptosis and efferocytosis. A large number of neutrophils in a diabetic wound and an increased neutrophil/lymphocyte ratio are well known as objective indicators of impaired diabetic wound healing [6-10]. Complete integral wound healing requires the combined interaction of numerous growth factors, cytokines and chemokines that play a vital role in the pathogenesis of the wound process. The most studied factors that contribute to the disruption of the wound healing in patients with DM in the case of chronic inflammation are interleukins IL-1β, IL-6, tumor necrosis factor (TNF-α), and plasma C-reactive protein [11-15].
The mechanisms of molecular interaction between neutrophils and monocytes/macrophages in the case of chronic inflammation require further study.
The objective is to study the profile of cytokines and eicosanoids in patients with neuropathic and neuroischemic forms of diabetic foot syndrome (DFS) complicated by DFU.
We examined 40 patients of two groups: those with DM2 complicated by DFU (group 1), with neuropathic (1A subgroup, n=10) and neuroischemic (1B subgroup, n=10) forms of DM2, as well as with DM2 without DFU (group 2), with neuropathic form (2A subgroup, n=10) and neuroischemic (2B subgroup, n=10) form of DM2. The neuropathic nature of DFU was diagnosed based on the verification of peripheral sensorimotor neuropathy with intact/slightly impaired main blood flow (ankle-brachial index (ABI) on both legs 0.9). The neuroischemic form of DFS included patients with defects in the integumentary tissues on the feet, accompanied by disturbances in the main blood flow (ABI<0.5) and signs of peripheral sensorimotor neuropathy.
Patients of both groups had the similar area (3.1±1.7 cm2 and 3.0±1.4 cm2, respectively) and depth of the ulcer (on average 2.7±1.5 mm and 2.9±1.3 mm, respectively) of the foot tissues. The concentration of cytokines TNF-α, IFN-γ, IL-1β, IL-6 and IL-10 in the exudate of the ulcer discharge was evaluated on the first day of hospitalization before surgery using immunoenzymometric assay (OOO "Cytokin", St. Petersburg) in accordance with the manufacturer's instructions. To measure LTB4 and PGE2 levels we used competitive assays (Leukotriene B4 ELISA Kit and Prostaglandin E2, both from Cayman Chemical, Ann Arbor, MI) according to the manufacturer's instructions. Lymphocyte immunophenotyping (CD4+, CD8+) was performed by flow cytometry.
Statistical analysis of the obtained results was carried out using STATISTICA 6.0. The analysis of the normal distribution of quantitative data was carried out using the Shapiro-Wilk test. Student's t-test was used for independent samples. The significance of differences in quantitative data that do not assume the normal distribution was assessed using the Mann-Whitney U-test. For non-normally distributed quantitative data, we calculated the median, first and third quartiles (Me [Q1;Q3]). The significance of differences in qualitative data was assessed using the chi-square test. To assess differences, the critical level of significance was p<0.05.
Patients with neuropathic DM2 of subgroup 1A differed from those of subgroup 2A by a significantly increased IL-1β concentration (29.2 (17.5; 43.8) versus 15.1 (5.7; 40.2), respectively, p = 0.033), and also a significantly low IL-10 content (8.4 (3.3; 15.4) versus 31.7 (28.2; 35.6) in subgroup 2A, respectively, p=0.014), which indicates a possible imbalance of these interleukins in patients with DM2 complicated by DFU. The content of IL-6, TNF-α and IFN-γ in the exudate of patients of both subgroups did not differ. Fig.1.
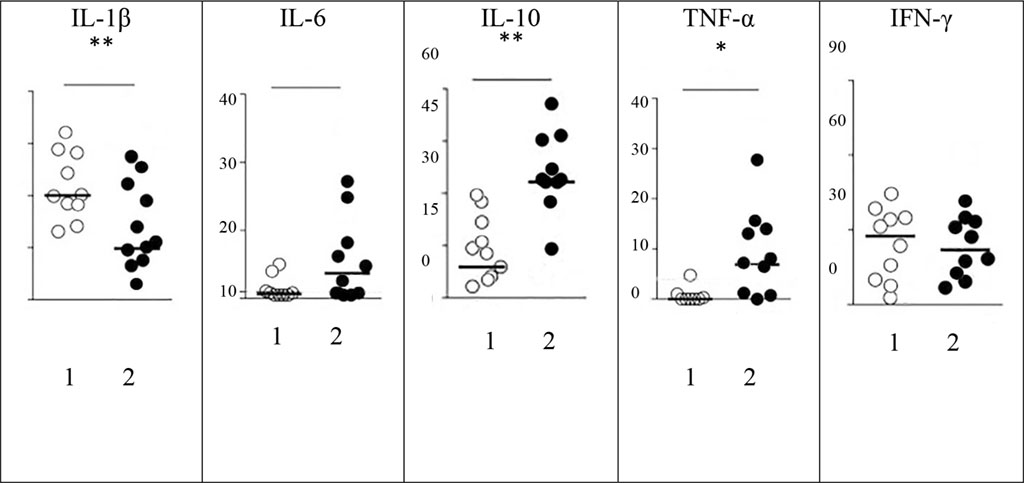
Figure
1. The level of cytokines (pg/ml) in the exudate of wound discharge
in patients with neuropathic DM2 (1) and DM2+DFU (2).
Note: 1 -
subgroup 1A, n=10, 2 - subgroup 2A, n=10. Here and in Figure 2: Data
are presented as a median. Mann-Whitney test. Statistical
significance * p < 0.05; ** p < 0.01.
Attention was drawn to the opposite pattern of the content of IL-1β in patients with neuroischemic form, which in patients with DFU exceeded the one in subgroup 1B: 95.6 (83.4; 105.1) versus 70.9 (58.3; 79 .4), respectively, with p=0.003. Concentrations of IL-6, IL-10 and TNF-α had similar to group 1 differences between uncomplicated form of DM2 and DM2 with DFU, while IFN-γ and IL-1β levels in neuroischemic form was higher in patients with DFU. Fig. 2.
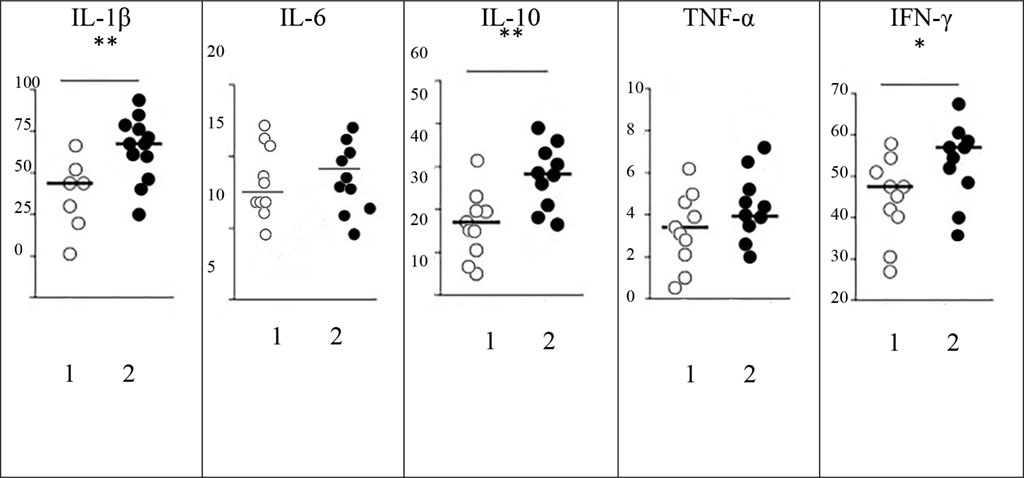
Figure
2. The level of cytokines (pg/ml) in the exudate of wound discharge
in patients with neuroischemic DM2 (1) and DM2+DFU (2).
Note: 1 -
subgroup 1B, n=10, 2 - subgroup 2B, n=10.
The revealed imbalance of cytokines in patients with DFU was manifested by a similar ratio of CD4+/CD8+. In both subgroups, CD4+/CD8+ increased to 2.3-2.5, however, in patients with neuropathic DM2, this was due to an increase relative to the number of CD4+, while in patients with neuroischemic form of the disease, it was due to a decrease in the number of CD8+.
Taking into account the scientific evidence on the participation of arachidonic acid metabolites (prostaglandin E2 and leukotriene B4) and their crucial role in the initiation of inflammation and the regulation of the immune response, hematopoiesis and M1 (pro-inflammatory) assistance to macrophages, we analyzed the content of these mediators in the exudate of the wound discharge of the examined patients. In patients with a neuropathic DM2 with DFU (subgroup 2A), the PGE2 level was significantly lower than that in patients of subgroup 1A - 161.4 (145.3; 173.8) versus 298.1 (260.3; 321.1), respectively, p=0.017. Patients with neuroischemic form (subgroup 2B) had a different picture: in the presence of DFU, the level of PGE2 exceeded that in subgroup 1B (335.8; 304.6, 367.7 vs. 210.9; 183.3, 234, 9), p=0.028. The content of LTB4 in the exudate of the wound discharge showed an inverse relationship. Thus, the formation of DFU in patients with the neuropathic form was manifested by a significant increase in leukotriene production, and in patients with the neuroischemic form - by inhibition of LTB4 secretion. At the same time, the balance of eicosanoids was disturbed and inconsistent.
The critical regulator of the neutrophilic phase of the inflammatory response is protein kinase C-delta (PKCδ), which activation is controlled by lipopolysaccharide (LPS), TNF-α, and IL-1β [16]. In addition, studies by Soroush F. et al. [16] showed an important role of PKCδ in TNF-mediated O2 production in human systemic neutrophils through PKCδ association and phosphorylation of the p47phox component of the NADPH oxidase enzyme complex.
As shown by the results of our study, the leading pathogenetic factors of the inflammatory and reparative process in the tissues of the foot with neuropathic 2DM+DFU are TNF-α and IL-6 hyperproduction. The identified features of the cytokine profile in patients with neuropathic DFU can be explained by the influence of eicosanoids in the regulation of the transition from the inflammatory phase to the proliferative one. In addition to inflammatory cytokines, resident tissue cells and migrating neutrophils of patients with neuropathic DFU produce excess lipid mediators, first of all LTB4, the main factor in the sustained response of neutrophils.
We found an overproduction of IL-1β in patients with neuroischemic DM2+DFU. The IL-1β mediated mechanism aims to trigger a feedback loop by activating macrophages, dendritic cells, γδ T cells, and endothelial cells to produce and release chemokines, and drawing more neutrophils. The overproduction of IL-1β in this category of patients may result in stimulation of CD4+ cells aimed at the secretion of IL-10, IFN-γ, and IL-2. IFN-γ producing CD4+ cells and PGE2 are required to control invading microbial inflammatory stimuli in order to initiate and maintain a mononuclear inflammatory response. The high production of IL-1β Nf in the wound in the presence of bacterial lipopolysaccharides ensures the differentiation of M2b type macrophages. M2b macrophages are designed to reduce inflammation by releasing anti-inflammatory cytokines as well as several different matrix metalloproteinases. However, judging by the multidirectional response of cytokines (IL-10, IL-6, IL-1β and TNF-α) in patients with ischemic DM2, the resulting imbalance of cytokines does not allow creating conditions for the differentiation of M2b macrophages. One of the reasons for this phenomenon may be impaired phagocytosis, since there is evidence that in vitro macrophages adopt the M2b phenotype after phagocytosis of neutrophils [17-19].
Thus patients with neuroischemic DM2 develop prerequisites for impaired transition of diabetic wound macrophages from pro-inflammatory M1 phenotypes to anti-inflammatory pro-regenerative M2 phenotypes, which is a key problem in the dysregulation of diabetic wound healing. It is critical that neutrophil activity should be strictly regulated to prevent excessive off-target damage to healthy tissue while protecting the host from pathogens.

|
||