- Home
- About the Journal
- Peer Review
- Editorial Board
- For Authors
- Reviewer Recognition
- Archive
- Contact
- Impressum
- EWG e.V.
Cite as: Archiv EuroMedica. 2024. 14; 4. DOI 10.35630/2024/14/4.412
Aims: This study aims to evaluate the efficacy and safety of tirzepatide, a dual agonist of glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptors, in promoting weight loss in patients with obesity.
Methods: A comprehensive literature review was conducted using PubMed and Google Scholar databases for articles published between 2020 and 2024. Keywords included tirzepatide, LY3298176, tirzepatide obesity, tirzepatide side effects, and tirzepatide adverse effects. Studies included were randomized, placebo-controlled, and involved patients with a body mass index (BMI) ≥ 30 kg/m² or ≥ 27 kg/m² with at least one weight-related comorbidity.
Results: Analysis covered 5,385 participants from phase 2 and 3 trials, with 3,517 treated with tirzepatide and 1,868 receiving placebo. Tirzepatide demonstrated significant weight reduction across studies: SURMOUNT-1 (15.0%, 19.5%, 20.9% weight loss for 5, 10, 15 mg doses respectively), SURMOUNT-2 (12.8%, 14.7% for 10, 15 mg doses), NASH SYNERGY (10.7%, 13.3%, 15.6% for 5, 10, 15 mg doses), and SURMOUNT-OSA (17.7%, 19.6% for maximum tolerated dose). Adverse effects were mostly gastrointestinal, with nausea, diarrhea, and vomiting being the most common, leading to a discontinuation rate of 4.6%.
Conclusions: Tirzepatide demonstrates superior efficacy in weight management compared to existing treatments, with an acceptable safety profile. Its dual agonist action offers a promising therapeutic option for obesity, warranting further research into its long-term benefits and impacts on obesity-related comorbidities.
Keywords: tirzepatide; obesity; GIP receptor agonist; GLP-1 receptor agonist; tirzepatide safety; incretins
Obesity is a widespread, multifactorial disease involving the excessive accumulation of body fat and is diagnosed when body mass index (BMI) equals or exceeds 30 kg/m². The pathogenesis of obesity is primarily driven by an excessive supply of calories in relation to energy expended; however, genetic and epigenetic factors have also been recognized as important [15, 9]. The incidence of this condition is steadily increasing [27, 14], posing an increasing challenge to the health of society due to the consequences it entails. Obesity is associated with an increased incidence of many diseases, such as type 2 diabetes mellitus, hypertension, hyperlipidemia, cardiovascular diseases, non-alcoholic fatty liver disease, cancers, chronic kidney disease, obstructive sleep apnea, and depression [27, 6, 30]. Depending on the degree and comorbidities, obesity can lead to a shortened life expectancy of 2 to 20 years [4]. Fortunately, we now have more therapeutic options at our disposal to tackle this condition. Scientifically proven methods to combat obesity include bariatric surgery, endoscopic interventions, lifestyle changes, and pharmacotherapy [7]. The recent discovery of highly effective substances for treating obesity marks a breakthrough in managing this disease, one of them being tirzepatide, a dual agonist of glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptors.
This article is a literature review based on publications from the PubMed and Google Scholar databases, published between 2020 and 2024. Using phrases such as: tirzepatide; LY3298176; tirzepatide obesity; tirzepatide side effects; and tirzepatide adverse effects, we obtained 354 results after excluding repetitions. The next step was content verification, research methodology evaluation, and sample size assessment. We only included studies involving patients that met the criteria for inclusion of pharmacological treatment—BMI exceeding 30 kg/m² or 27 kg/m² with at least one weight-related comorbidity. Despite the different objectives of the analyzed studies, we focused on the impact of tirzepatide on weight reduction, with varying drug doses and various accompanying therapy factors.
Tirzepatide is a long-lasting dual GIP and GLP-1 receptor agonist from the incretin mimetics group. The molecule has an affinity comparable to native GIP for the GIP receptor (GIPR) and approximately five-fold weaker than native GLP-1 for the GLP-1 receptor (GLP-1R); however, action through both incretin pathways is crucial for the effect [5]. GIPR and GLP-1R are found in many different tissues, such as pancreatic α and β endocrine cells, heart, neurons, vasculature, leukocytes, gut, and kidney. GIP receptors are also present on adipocytes [22]. This results a multidirectional mechanism of action for this drug. The effects of the drug include improved glucose-dependent insulin secretion, glucose tolerance, insulin sensitivity, and markers of pancreatic beta-cell function [5, 28, 1]. Non-glycemic mechanisms significantly contributing to the effects of weight reduction include delayed gastric emptying, appetite suppression, and improved satiety leading to lower caloric intake. The weight reduction is mainly attributable to the reduction of body fat [11].
The studies described in this text were phase 2 (NASH SYNERGY) or phase 3 (SURMOUNT 1-4, SURMOUNT-OSA) randomized, placebo-controlled, multicenter, double-blind clinical trials [15, 18, 17]. The primary inclusion criteria for participants ensured that all patients involved had a BMI ≥ 30 kg/m² or ≥ 27 kg/m² with at least one weight-related complication [13, 10, 29, 2, 18, 17]. The differences in additional inclusion criteria and accompanying factors among the analyzed studies allowed observation of tirzepatide's impact on weight reduction in conditions similar to daily clinical practice. However, appropriate selection based on common characteristics enabled the comparison of these studies and the drawing of common conclusions from them.
Some studies divided patients into groups based on the dose of tirzepatide they received [13, 10, 17]. The aim of the SURMOUNT-1 study was to examine weight reduction depending on whether the dose was 5, 10, or 15 mg of tirzepatide weekly [13]. Similarly, the SURMOUNT-2 study specified groups receiving 10 and 15 mg of tirzepatide weekly [10]. The main difference between these studies was the presence of type 2 diabetes in participants. SURMOUNT-1 excluded such patients, while SURMOUNT-2 included them [13, 10]. The NASH SYNERGY included patients with or without diabetes, aiming to demonstrate tirzepatide's impact on the resolution of NASH without worsening fibrosis. However, due to patient selection, it also provided valuable information on the effect of tirzepatide on weight reduction in obese patients. It divided patients into groups receiving 5, 10, and 15 mg of tirzepatide weekly [17].
In other studies, participants received the maximum tolerated dose (MTD) of tirzepatide, either 10 or 15 mg, and their group division was determined by factors other than the dose received [29, 2, 18]. The SURMOUNT-3 trial investigated the impact of tirzepatide MTD on body weight change in participants who achieved ≥5.0% weight reduction after a 12-week intensive lifestyle intervention, combining reduced caloric intake and physical exercise [29]. The SURMOUNT-4 trial aimed to determine the difference in weight loss among participants treated with tirzepatide MTD for 88 weeks versus those treated with tirzepatide MTD for 36 weeks followed by a placebo for the next 52 weeks [2]. SURMOUNT-OSA divided participants into those not receiving positive airway pressure treatment at the beginning of the study (group 1) and those receiving such treatment (group 2). Both groups also received tirzepatide at the maximum tolerated dose [18].
In all studies, tirzepatide doses were introduced gradually, starting at 2.5 mg per week, increasing by 2.5 mg every 4 weeks until the target dose was reached [13, 10, 29, 2, 18, 17]. SURMOUNT 1-4 and SURMOUNT-OSA included the addition of a daily calorie deficit of 500 and a minimum of 150 minutes of physical activity per week in the therapy [13, 10, 29, 2, 18]. The studies included participants with various types of weight-related complications, such as type 2 diabetes, obstructive sleep apnea, hyperlipidemia, NASH, hypertension, and others.
The studies analyzed included a total of 5,385 participants, of whom 3,517 were treated with tirzepatide and 1,868 were receiving a placebo. When comparing, it is important to consider the different durations of the studies from which conclusions were drawn.
The studies comparing the effectiveness of different doses of tirzepatide showed the following results. The SURMOUNT-1 trial showed, at week 72, an average body weight loss of 15.0% with 5-mg weekly doses of tirzepatide, 19.5% with 10-mg doses, and 20.9% with 15-mg doses. The placebo resulted in a body weight reduction of 3.1% [13]. In the SURMOUNT-2 trial, evaluated after 72 weeks, the mean change in body weight was -12.8% with a 10-mg weekly tirzepatide dose and -14.7% with a dose of 15-mg, while -3.2% with a placebo [10]. The NASH SYNERGY trial at week 52 with doses of tirzepatide of 5, 10, and 15 mg per week resulted in a weight reduction of 10.7%, 13.3%, and 15.6%, respectively. The placebo led to a decrease in body weight of 0.8% [17].
In the SURMOUNT-OSA study, tirzepatide at the Maximum Tolerated Dose (MTD) resulted in a weight reduction of 17.7% in group 1 and 19.6% in group 2 at week 52 of the study. The results for the placebo groups were 1.6% and 2.3%, respectively [18]. In two subsequent studies, the maximum tolerated dose of tirzepatide was also used. However, due to a more specific pre-randomization and open-label lead-in period, these results stood out compared to those presented above. In the SURMOUNT-3 study, the average change in body weight prior to randomization was -6.9%. Following randomization, the group receiving tirzepatide at the maximum tolerated dose for 72 weeks experienced further weight reduction of 18.4%, while the placebo group recorded an average regain of 2.5% [29]. In the SURMOUNT-4 study, after 36 weeks of tirzepatide therapy at the MTD, participants achieved an average weight loss of 20.9%. Upon dividing into two groups, participants who continued with tirzepatide experienced a further weight change of -5.5%, while those who started taking a placebo after the 36-week therapy saw a regain in weight of 14%. The overall mean weight reduction throughout the study was 25.3% for tirzepatide and 9.9% for the placebo [2].
During the clinical trials considered, tirzepatide was well tolerated. Approximately 4.6% of participants dropped out due to adverse effects, including those in the placebo group. The following adverse events led to discontinuation: nausea, diarrhea, abdominal pain, vomiting, and very rarely, an increase in pancreatic enzymes. Approximately 76% of patients participating in the trials reported at least one adverse symptom. In the obese population, gastrointestinal side effects were most common and included nausea, diarrhea, constipation, vomiting, and dyspepsia [2, 10, 13, 17, 18, 29]. Based on data from the SURMOUNT-1 study, these accounted for 51.3%, 55.2%, and 55.6% of patients for the individual doses of 5 mg, 10 mg, and 15 mg, respectively, compared with 28.5% in the placebo group [13].
During the SURMOUNT-3 trial, the use of antiemetic drugs was reported by 78 participants (27.2%) treated with tirzepatide and 20 (6.8%) treated with placebo. The use of antidiarrheal medication was reported by 23 participants (8.0%) treated with tirzepatide and by six (2.1%) treated with placebo. The reason for the increase in adverse events may be due to the intensive lifestyle intervention. Patients receiving tirzepatide in the SURMOUNT-3 trial, compared with the group receiving tirzepatide 15 mg in the SURMOUNT-1 trial, had moderately higher rates of gastrointestinal adverse events. It is speculated that calorie restriction may lead to a decrease in GLP-1 in the gastrointestinal tract, which may worsen initial gastrointestinal tolerance to incretin-based therapy; this is a possible explanation for the observed results but requires further study [29].
The incidence of adverse effects increases during the period of dose escalation. These effects were more frequent in the tirzepatide group than in the placebo group. The symptoms were transient and ranged from mild to moderate severity [2, 10, 13, 17, 18, 29]. Serious adverse events were reported by approximately 6.1% of participants, described as similar in frequency between tirzepatide and placebo groups. Pancreatitis cases confirmed through assessment were evenly distributed among all treatment groups, including the placebo group, with none classified as severe. The occurrence of cholelithiasis, cholecystitis, and acute cholecystitis was similar between the tirzepatide and placebo groups [2, 10, 13, 17, 18, 29]. A total of 17 deaths were reported during the study. None of these deaths were considered by the investigators to be related to the study drug. There is also no evidence linking the use of the drug to the occurrence of malignancy [2, 10, 13, 17, 18, 29].
The data on adverse effects acquired during the SURMOUNT 1-4, OSA, and SYNERGY NASH studies have been collated and are presented in the Table 1 below.
Table 1. Summary table of adverse effects reported during SURMOUNT 1-4, SURMOUNT-OSA and SYNERGY-NASH clinical trials
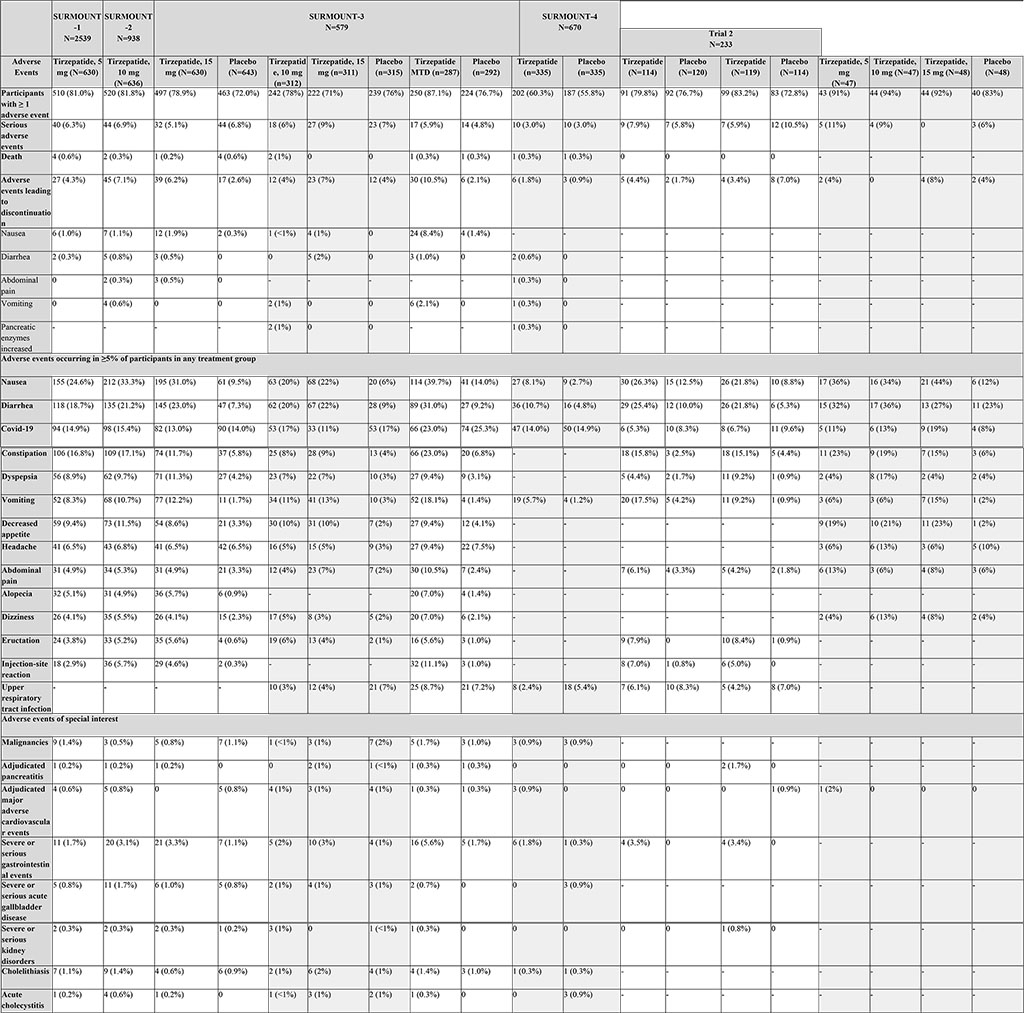
The tables with summaries of adverse effects from each study have been combined into one .If a particular type of adverse reaction was reported in one study and did not represent a significant percentage, it was omitted to maintain transparency for the viewer.
In all studies, tirzepatide outperformed placebo and showed a significant and statistically meaningful reduction in body weight in patients with obesity. We did not include studies such as SURPASS-1 in our analysis because it also allowed participants with a body mass index within the normal range. However, it should be noted that this study also showed a significant weight reduction, reaching 11% after 40 weeks of tirzepatide therapy. The trial involved patients with type 2 diabetes inadequately controlled by exercise and diet alone [21]. It is worth mentioning ongoing studies such as SURMOUNT-5, which compares the effectiveness of tirzepatide and semaglutide in weight reduction in patients with obesity or overweight and at least one weight-related comorbidity, who have a history of unsuccessful dietary efforts to lose body weight [25]. The SURMOUNT-J study is also currently testing the effectiveness and safety of tirzepatide in patients with overweight and obesity. Further research is needed to explore the long-term effects on obesity-related comorbidities [24]. Three other ongoing studies have more narrowly defined criteria regarding comorbidities. The TREASURE-CKD trial aims to assess the potential benefits of using tirzepatide in patients with chronic kidney disease [26]. Meanwhile, the SUMMIT trial focuses on patients with heart failure in NYHA class II-IV with preserved ejection fraction [23]. Both studies include entry criteria of a BMI of at least 27 and a BMI of at least 30, respectively [26, 23].
The data suggest that while tirzepatide is associated with an increased risk of adverse events, particularly gastrointestinal issues, it does not significantly elevate the risk of more severe outcomes such as death or major adverse cardiovascular events. The health benefits of continued tirzepatide treatment during the mentioned trials were achieved with a safety profile consistent with that previously reported in the SURPASS trial and in trials of incretin-based therapies approved for the treatment of obesity and overweight [2, 10, 13, 17, 18, 29].
When compared to existing weight management therapies, tirzepatide shows superior efficacy. The weight loss achieved during its usage is higher compared to GLP-1R agonists [1]. The dual receptor agonism of tirzepatide, due to probable potentiation of action within GLP-1R with GIPR agonism, may have an advantage over single-receptor agents by targeting broader metabolic pathways.

|
||